This is the moment at least two of you have been waiting for for almost a year! See also the previous post if you’d like to compare.
Page visits
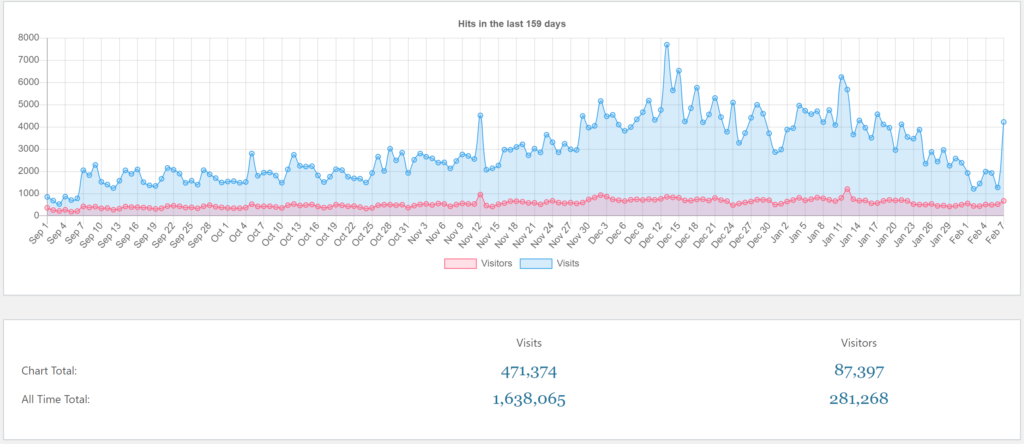
As usual, a page “visit” refers to opening a single page on greek.doctor. A “visitor” is a unique person within that day.
These are the page visits for this semester, which began at September 7th, and a few days preceding it. Not surprisingly, the numbers are lower in the days preceding the semester, at around 200 visitors and 800 visits per day. Then, the semester began at September 7th, after which visitors numbers and visits suddenly increase to around 400 visitors and 2000 visits.
There is a very nice sinusoidal pattern in the first weeks of the semester, with much higher visitor numbers and visits on Monday – Wednesday, with numbers dropping off the rest of the week until the next Monday.
Visitors and visits remain relatively stable in the first 7 weeks, as people are generally on low gear in the first half. Classically, people start panicking around the 7 week mark, after which a higher gear is assumed.
There is a small peak at November 12th, but I don’t know why. I don’t have good insight into which pages were actively used during that day, but I think pathophys pages were most active. Could it be the day before pathophys 1 midterm? Was there even a midterm this semester?
Page visits peaked during this period on December 13th, at 7701 visits, the day before the beginning of the exam period. I’m certain that more cramming of information occurs on this day than on any other day of the exam period or semester. And then, in the afternoon hours of December 14th, most of the information was probably forgotten.
Page visitors peaked on January 12th, for reasons I don’t know. There were 1204 visitors that day.
Numbers were low at December 31st and January 1st, at 3000 visits and 500 visitors.

Since last post, we’ve passed 1 000 000 page visits, and we’re already over half way to 2 million!
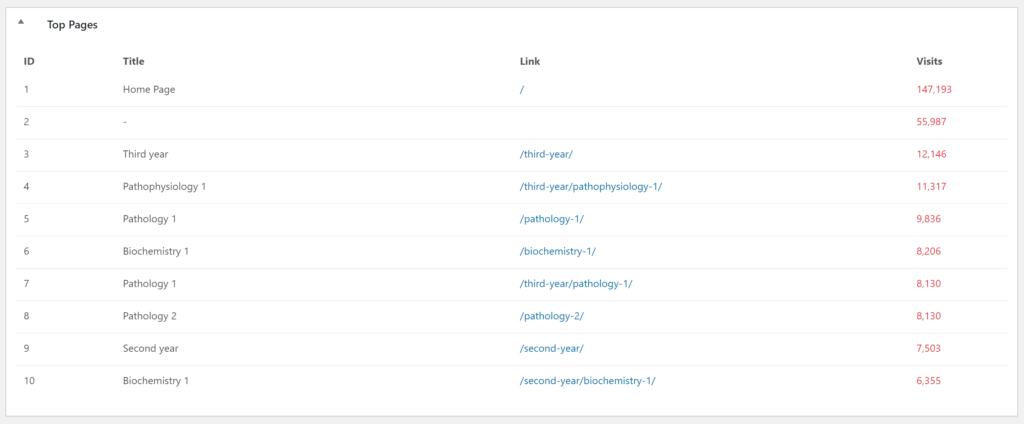
I think it’s safe to say that the notes for third year subjects are the most popular. These numbers only account for the visit to the parent pages of each subject, not the child pages of each subject. The results are kind of messed up because I moved all subjects to their respective years sometime during the summer (I think?), which is why you see both /pathology-1/ and /third-year/pathology-1/ in this list, even though they’re the same page.
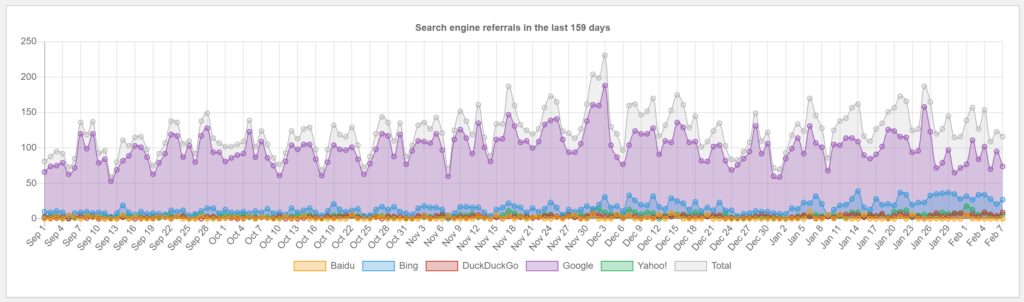
Looking at the number of page visits from search engines is fun, because there’s a much smaller correlation between them and the semester at POTE than there is for other metrics. I assume this is because most POTE students don’t use a search engine to find greek.doctor. Most search engine referrals are from people searching for medical terms and ending up here.
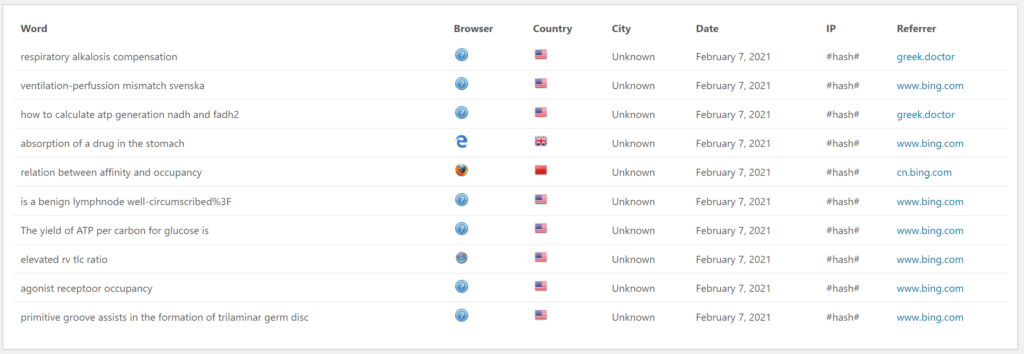
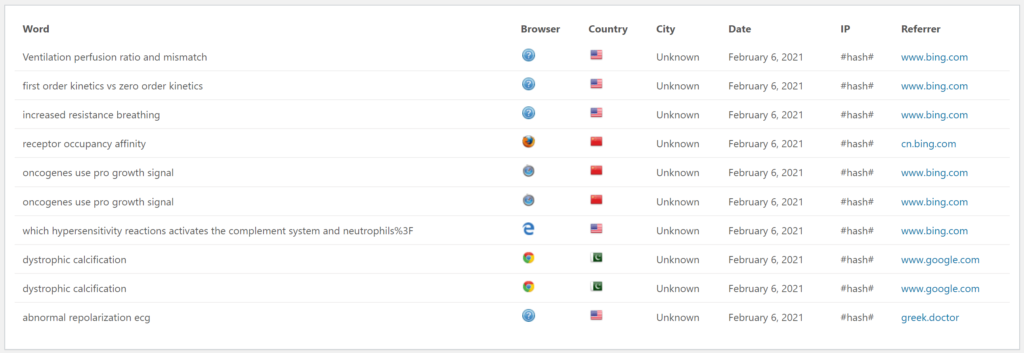
There are the last 20 search words people used before ending up at greek.doctor. This is one of my favourite metrics; I love looking at what people are looking for before ending up here. I hope they find what they’re looking for.
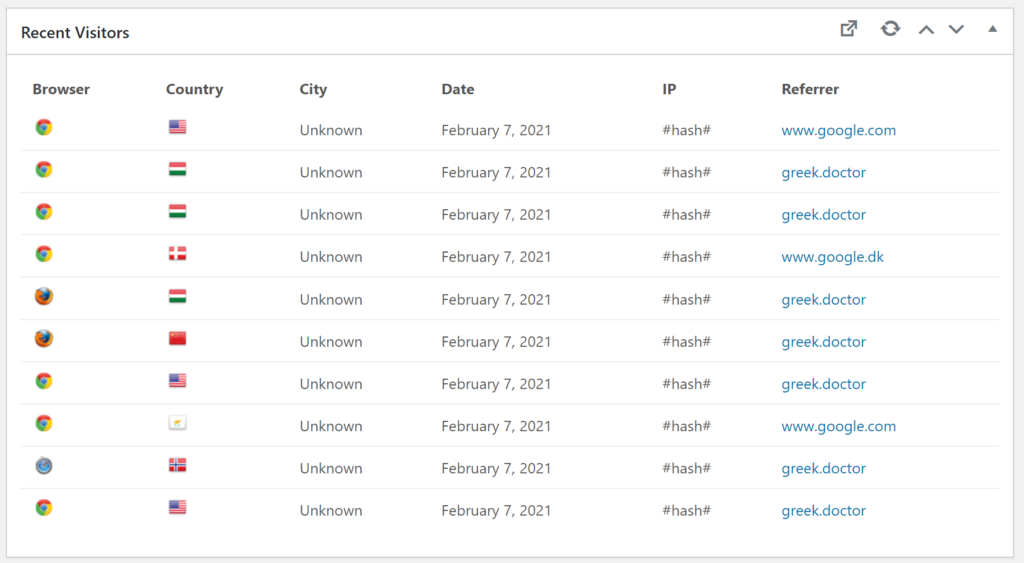
These are the countries from where the last 10 visitors were from. There is a bit of variety, which is cool!
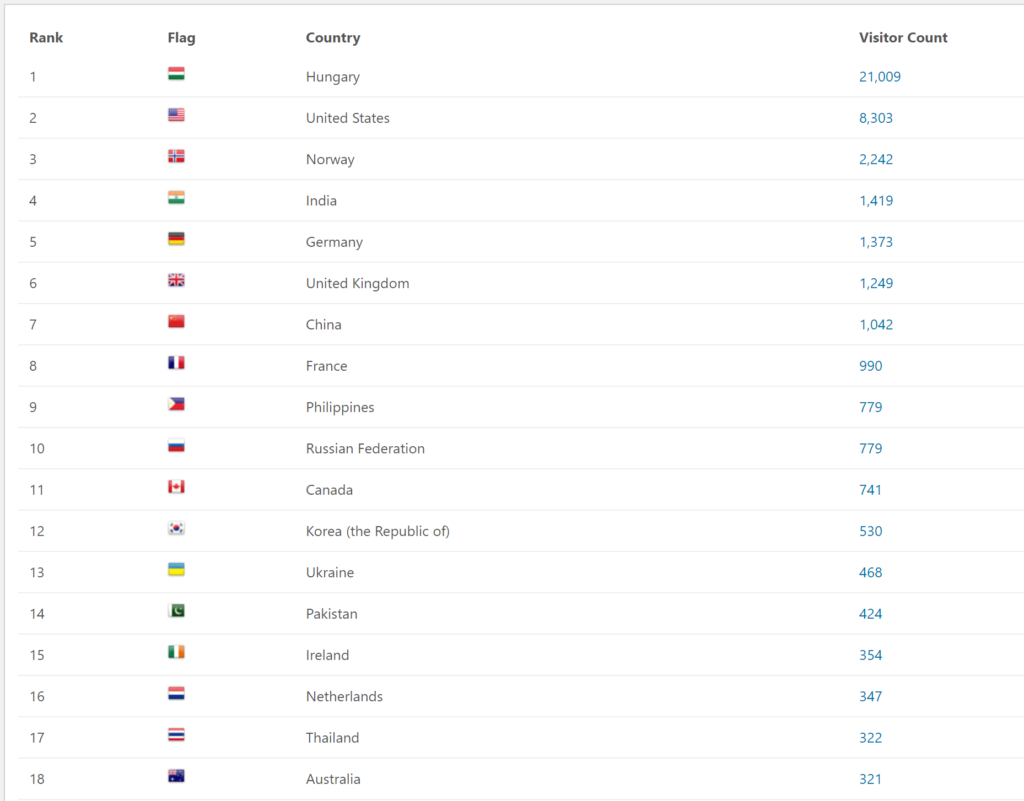
This list shows the number of visitors from each country during the semester.
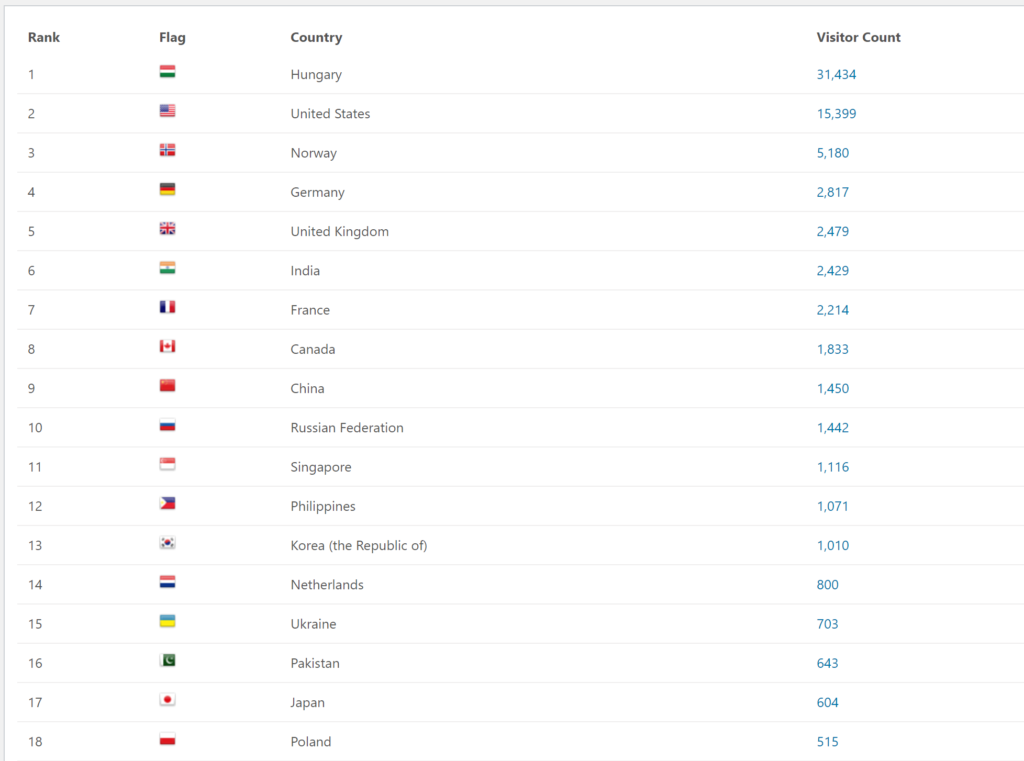
This list shows the number of visitors from each country during the exam period. It’s very interesting to see the large variety, although it’s no shocker to see that Hungary is at the top by a large margin. Hungary would probably have won by an even larger margin if most of us didn’t travel home to have our online exams from home.
Comments
It’s time for a few comments! There are now 1362 comments, of which 600 are mine, leaving 762 comments for others.
Results of maintainance
Maintainance went pretty smoothly. Some technical jargon ahead:
The server was running ubuntu 16.04, which was EOL soon (April?). It’s now upgraded to 20.04, which is supported for 4 more years. I’ve also hardened the server a bit. I was planning to make a good automatic backup solution during the maintainance, but there wasn’t enough time for me to finish it. That shouldn’t require downtime, though.
Next semester
I don’t know which subjects I’ll write notes for this semester yet. I’ll let you know, though.