Happy new year!
Had ENT yesterday. I studied 4 days of it, but those days included new years, so it was more like 3 days of effective studying. It has multiple practial parts and one theroretical part. There are separate examiners for the practical and theoretical parts. We waited at the entrance of the department until a teacher called us in 15 minutes later.
Practical parts
They took 2 and 2 students in to an examination room in the ambulatory unit. They brought in a healthy-looking patient for the examination. There are two doctors in the room, both are young doctors, one male and one female. The male was our primary examiner for the practical part, the female was the co-examiner.
The primary examiner takes out a bowl containing many instruments related to ENT. “Let’s talk about myringotomy”, he tells me. He asks me many questions, like:
- In which quadrants can we perform myringotomy?
- What are the indications for myringotomy?
He also takes out a myringotome and a grommet (it’s very small and comes in a blue box), and asks me what they’re used for. I mess up a lot on this part, mixing serous and suppurative otitis media and stuff. He still gives me a 4 at this part.
Next, he asks me to examine the patient’s neck. I start by palpating the retroauricular and preauricular lymph nodes, and I continue palpating the other lymph nodes, before he stops me and asks the names of the different lymph node regions, and which cancers drain into which regions. He also asked me the borders of the posterior triangle.
I make a lot of mistakes here, especially regarding the cancers. I call regions II, III and IV the upper, middle and lower internal jugular chains (which multiple other sources call them..), but he says that they’re called the parajugular regions. He gives me a 3/4 here. I never got to finish the neck examination, and I never examined the patient with a headlight.
Theoretical part
The theoretical part begins by you having to write down the top ten. I write down 9, but of course I forget the last. The male examiner from before takes my paper and looks at it, before he asks “What about hoarseness?”, and I suddenly remember the last one (the 3 weeks hoarseness one).
I’m then taken into an office, where I draw a topic and sit down to prepare. My topic was “Fluid systems of the inner ear, Meniere’s disease and toxic lesions of the inner ear”. Ps: the topics were in order, so that
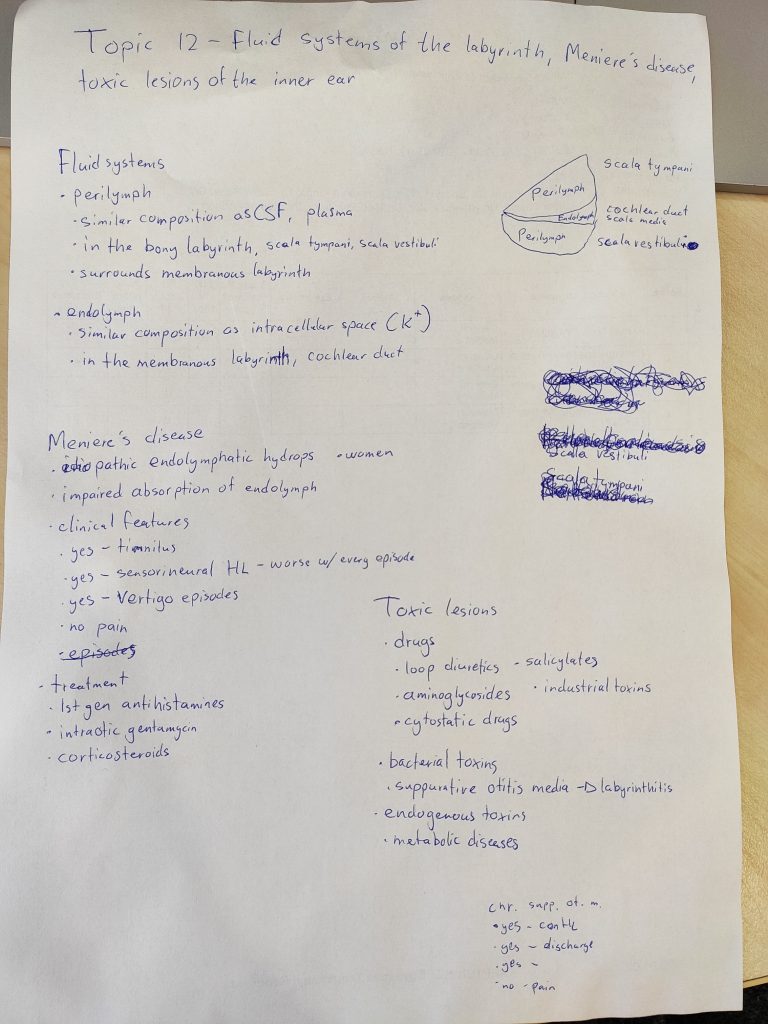
After some preparation the man himself comes in. I start with my topic, explaining what I had written down about the endolymph and perilymph (not mentioning the drawing on the right, because I wasn’t totally sure about it). He has no questions there, so we move on to Meniere’s.
I explain what I had written down (I had the “no” wrong, I just noticed. He didn’t comment that). He asks me how to diagnose it. I tell him that you need a certain number of attacks within a certain time-frame, but I don’t remember the specifics. He asks me about other potential treatments. I don’t know any more, I tell him. That brings out the asshole in him.
- “When you study a disease, do you just read about the symptoms and the pathophysiology and skip the diagnosis and treatment? If a patient comes in with this disease, they’re not interested in the pathophysiology, they’re interested in how you can treat them. What are you going to tell your patient when you don’t know how to treat them?
- “How long did you study for this?”
- “Where did you study from?” “The Thieme book” “Are you telling me that the book doesn’t write about the diagnosis and treatment of Meniere’s disease?”
- “Everyone with this topic just mentions the three yes and one no and thinks that’s everything which is important”
I wish I told him to fuck off there and then, but that’s easy to say in retrospect I guess. Like, bitch, nobody retains everything they read, and if there’s something I don’t know as a doctor I would just look it up anyway. He was rude to the other students as well.
We move on to the toxic lesions. I mention what I had written down. He asks me for examples of metabolic diseases which can damage the inner ear. I didn’t know any examples so I guessed diabetes (always a good guess), which was appearently correct. He also mentioned uraemia.
He then asks me what the “three yes and one no” of chronic suppurative otitis media are. I remembered only two yes and one no (I forgot the perforated tympanic membrane), but when he asks “what causes there to be otorrhoea?” I remember the last yes.
He then asks me the four major symptoms of chronic rhinosinusitis. I spend some time thinking, and I recall three of them. “You forgot the most important one” he says, at which point I remember “nasal airway obstruction”.
He gives me a 3 in total, further dissing me for “skipping” the diagnosis and treatment when studying.
My tips to you would be to know the pathophysiology, symptoms, diagnosis and treatment of each disease, and definitely know the “three yes one no” for Meniere and chronic suppurative otitis media, the four major symptoms of chronic rhinosinusitis and of course the top ten (you can’t draw topic if you don’t know them).
The younger examiners were very nice and helpful though, even though I was grilled by the male one. Both examiners were in the room when I was examining the patinent, and I think they would help out with the hungarian if that would be a problem.
Next
Next is radiology written the 10th. It will be the first exam this exam period where I have enough time to maybe take it a little bit easier, which I’m looking forward to.