I had my neuro 2 exam today. The exam would start at 9 according to neptun, but the day before we got an e-mail that it would start at 8 instead. The exam was at the rehabilitation clinic next to the neurology department. The examiner was my teacher in Neurology 2, the course director of the subject, prof. Endre Pál.
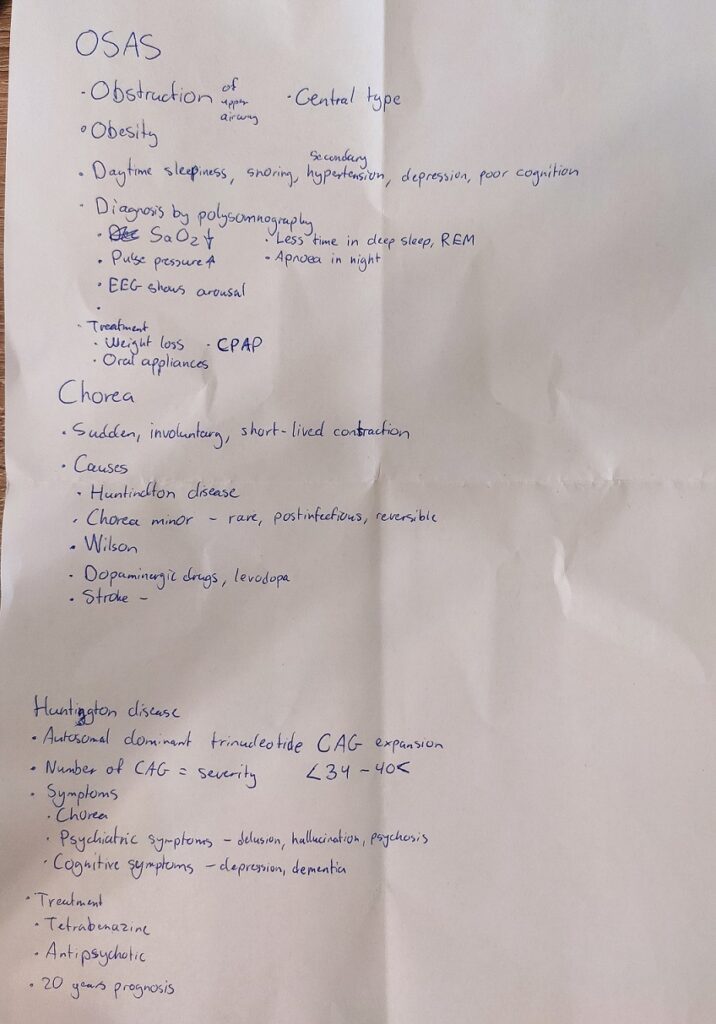
I was one of the last persons to go in. I draw topic 28, with obstructive sleep apnoea syndrome and Huntington disease. We got a few minutes preparation time if we wanted, during which I made this:
28A. Obstructive sleep apnoea syndrome
I mentioned what I’d written down about OSAS. He asks about two indexes which are measured during polysomnography. I guessed one of them, the apnoea index. He told me that the other one is the oxygen saturation index. I don’t think I had any other questions on this topic.
28B. Chorea, Huntington disease
I begin by defining chorea, and mentioning the most common causes. He asks me what a stroke-induced chorea looks like, and I said hemichorea, which was correct.
I then talk about Huntington, just basically what I’d written down. He asked me which diseases it’s important to rule out in case of Huntington, and he remembered he’d mentioned in the seminar that it’s important to rule out Wilson and Parkinson. He asked how we could do that, and I answered serum/urine copper and ceruloplasmin for Wilson. For Parkinson I said SPECT or PET, which he said was a possibility. He asked me what Parkinson disease patients respond to, and I answered levodopa, which was correct. He said that in ambigous cases we could give levodopa to the patient. If the symptoms improve, it’s PD, if they worsen, it’s HD.
He asked me what anticipation was, which was funnily enough something I learned in genetics two weeks ago. I explained that it means that the disease becomes worse and worse with each generation, to which he agreed. He asked me a couple of other questions as well, but I don’t remember what. In the end he gave me a 5.
Finishing thoughts
Prof. Pál is a very kind person, a good teacher, and an excellent examiner. The atmosphere of the exam was calm, he was not strict, and I’m pretty sure he passed everyone that day.
So I had my A&IC exam today. It was a bit of an experience, especially an unexpected one. I’d heard that the exam is with no prep time and just 5 minutes, but the exams today were with preparation time and they took much longer than 5 minutes.
I’m not sure who the examiner was, but after looking at the department site I think it was Dr. Tamás Kiss. I don’t know who the co-examiner was.
Me and two Hungarian students enter the K001 seminar room at 400 bed clinic at 9:00, and we’re told to sit down with some distance. They ask who wants to start, and we agree amongst ourselves that I should start. I draw two topics from separate envelopes. I get:
14. Mental disorders, drug overdosed patients (the unconscious patient and toxins)
4. Pharmacology of inhalational anaesthetics
I expected to start the exam right away, but instead they gave me the paper to start preparing, which was a surprise. I hadn’t even brought a pen because I thought there wouldn’t be prep time. Anyway, I start preparing.
Even though I started preparing first, one of the other student finished before me, and so started the exam first. Their exam was in Hungarian, so I couldn’t understand much of what they were saying. From what I gathered, he was talking about monitoring during anaesthesia, and there were some things he’d forgotten to mention and the examiner spent A LOT of time helping him remember them. I think his exam lasted around 40 minutes. During this time I was thinking of how different this exam is going to be from my expectations.
After a while it’s my turn. I begin with my first topic.
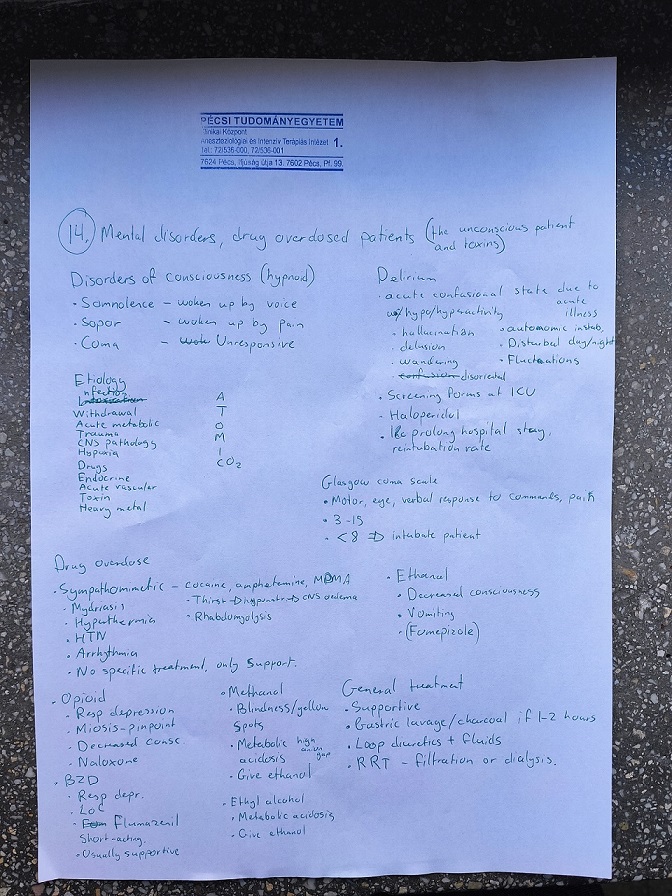
14. Mental disorders, drug overdosed patients (the unconscious patient and toxins)
I didn’t expect to upload photos of my prep papers ever again
I began by saying that I can talk about the disorders of consciousness, to which he agreed. I mention the three types. Then I talk about the I WATCH DEATH mnemonic, which I’m not sure I remembered correctly but I didn’t make any comments about it. I also talked about the GCS. He then asked me about a simpler way to scale the patient’s consciousness. I barely remembered (after some help) about AVPU, and he asked me what it stands for. I barely remembered that as well.
I say that I can talk a bit about delirium here as well, which he agrees to. He mention what I’d written down. He asks me about what can cause delirium in the ICU specifically, as opposed to other hospital wards. I guess lots of things, like infection, sepsis, shock, postop, etc., but he says he’s after “something much simpler”. “Think about the typical patient. Who are they?” I say “elderly”, and he’s like “yes! exactly, simply old age and dementia can cause it”. Then he’s after another thing as well. Eventually he tells me “What’s different in the ICU compared to other wards? What happens at 2 in the night in the ICU?”, at which point I understand that he was talking about sleep deprivation, which was correct. He says to move on to the next part, the drugs.
I begin with the sympathomimetics, and before I can mention the symptoms he asks me what the symptoms are. He then tells me to talk about opioids, and I mention what I’d written. He asks me about the respiratory pattern in opioid intoxication. I mention that it is very slow and shallow, which he degrees with. He says that it’s deep rather than shallow.
At this point he says he’s happy and that we should move on to the next topic. I never covered the other drugs.
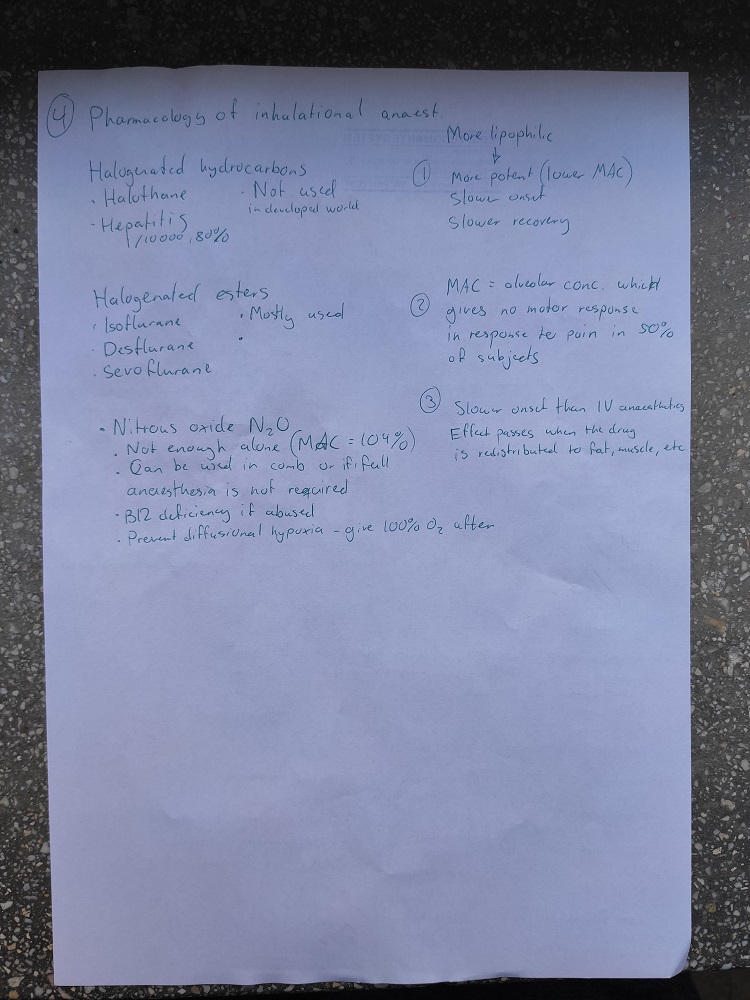
Pharmacology of inhalational anaesthetics
I’d even numbered the things so I knew the order of which to talk about stuff
I begin by mentioning that inhaled anaesthetics are lipophilic drugs, and the more lipophilic, the more potent, the slower the onset, and the slower the recovery. I tell him the definition of MAC, after which he stops me and tells me that MAC isn’t really a measure of potency, for some reason he explains to me which I don’t really understand. He then asks which alveolar concentration of anaesthetic we use in general anaesthesia, to which I reply “1,3 x MAC”. He say’s “1,2 – 1,3, correct”.
I then mention point 3, before I talk about halothane. I mention what I’d written, and I continue to the halogenated ethers. I didn’t remember any of the specific effects of them during prep, so I hadn’t written any down as you can see. I continue to nitrous oxide, and mention what I’d written. He asks me about which other effect N2O has, aside from the anaesthesia itself. I guess “analgesia”, which was apparently correct.
He asks about situations where we could use it in alone. I mention procedures like dental procedures or colonoscopies, but they weren’t really what he was after. He says “in which situation do you think it’s an advantage that the patient does not completely lose consciousness, but is pain relieved? Think of younger women”, at which point I guess “during labour”, which was correct.
He then circles back to halogenated esters, probably because they’re the most widely used but I didn’t mention a lot about them. He says that there are three effects of them on the body, and he wants me to mention them. I remember that they increase ICP, which was correct. He asks me how they do that, and I guess that they vasodilate cerebral arteries, which was correct.
He then says “if they vasodilate the cerebral arteries, what do you think happens with the other arteries in the body?” I guess that they vasodilate as well, potentially causing hypotension, to which he agrees. I say that they have a depressant effect on the heart, to which he agrees and then asks which of them have the least cardiodepressive effect. I had noe idea, so I guess one of them (don’t remember which one), but it was the wrong one. I don’t remember which is the right one.
He asks about the last effect. I don’t know, but he tries to help me by saying that it affects the respiratory system. I remember that some of them cause airway irritation, so that they can’t be used for induction of anaesthesia. He agrees, but that wasn’t what he was looking for. He asks me which of them that can be used for induction. I guess one of them, but it was wrong again. Don’t remember what I guessed or what was correct.
He’s still waiting for the third effect of these drugs. He tries to help me by saying that it’s a very useful effect in the ICU. I had a small hunch that it was bronchodilation, so I guessed it, and it was correct.
He asks me about which patients it’s preferred to use inhalational anaesthetics for induction rather than IV. I remember from the paediatric anaesthesia topic that it’s better for young children, which is what I tell him and he’s very happy. That was the end, and was very satisfied and gave me a nice 5.
Final thoughts
It was a very different experience from what I expected. I expected a short exam with no prep, not this. But he was very enthusiastic when I gave right answers, and he didn’t seem to mind wrong answers too much. He gave helpful hints and was patient, but perhaps a bit intense. I was kinda lucky because 1,5 of my topics was mostly pharma and the other half was mostly psych.
So I had nephro exam yesterday. It was very frustrating, not because of the exam itself but because of the lack of information and organization.
According to Neptun, the exam starts at 8:30 at the 2nd department of internal medicine. At 8:20, we enter and ask the secretery where to wait. She said that we should wait outside the entrance to the “A” building, at the lower level. At around 8:45, an employee comes and gets the first student. The first students is inside at least 45 minutes, which of course worries us greatly.
However, turns out that their examiner dr. Tibor Kovács, had been late. The exam itself lasted just 5 minutes (short questions and answers), the remaining time was just waiting for him. The next student goes in, and the same happens. They’re inside for 30 minutes, 25 minutes of which were waiting for the examiner (again), and 5 minutes of exam.
However, there were two examiners for English program that day, dr. Kovács and dr. Botond Csiky. Csiky examined Hungarian students too and no one told us that he would examine some of us international students as well. Turns out that three of us were part of dr. Csiky’s exam list, but no one had told us.
I wait and wait, and at around 10:30 I get a message from a kind international student, who were wondering if I was going to show up for my nephro exam today, which made me very confused of course, as I was waiting where I’d been told to. He tells me that I should come up to the third floor and wait for my exam there, where dr. Csiky was examining other students. Turns out my turn had already passed but no one had thought of checking if I was waiting outside the entrance.
Anyway, after two students before me finish their exams, I go in to do my exam. He tells me to talk about acute nephritis. At first I didn’t understand what he meant, but soon I understood that he meant tubulointerstitial nephritis so I start talking about that.
I say that it’s the inflammation of the tubules and interstitium, causing a decline in kidney function. I mention the most common causes, the clinical features, the findings in the blood and urine, and the treatment. Basically most of what I’d written in my topic.
He then says “okay, talk about poststreptococcal glomerulonephritis”. I begin by saying that it’s not as common nowadays because of antibiotics, but that it can occur after other infections, which is becoming more common. He asks me where the infection can be. I say tonsillitis or pharyngitis, and he says “and?”. “Rheumatic fever?”. “Not really. A skin infection”. Of course. Should have thought about that.
I continue, talking about nephritic syndrome, how it can be diagnosed, the antistreptolysin (ASO) titer, etc. He asks me about the treatment. “You treat the underlying infection with antibiotics”, I reply. “And?”. “I’m not sure?”
“And then you wait.”
Okay, I guess?
He then says that it was excellent and that I get a 5. It probably took less than 4 minutes. It was a nice experience, although he did not really give any feedback underway, which was a bit worrying.
My next exam is anaesthesia and intensive care on Tuesday.
The last of my 6 first week exams, the last card in the full house, was paeds 2. In the 10th semester there’s one opportunity for written paeds 2, which we’d discussed with the course director and we’d agreed that it’d be on Friday week 1, so everyone had it that day. According to the course director, it’d be an easy exam. According to another teacher, “something have to go completely wrong for you to fail it” or something. According to the email we got with information regarding the exam, the exam would ask the curriculum of “lectures and seminars” this semester, and not from last semester. The course director had also said this in the lecture. A major problem with this is that every group had very different seminars, teaching very different material.
The exam itself was a disaster. Each question was not marked with whether it was simple choice or multiple choice, and they told us at the exam that “we have to know” based on the answer options. There was no answer key, which is standard for written exams (1 + 2 + 3, 1 + 3, etc.).
There were also multiple questions related to last semester’s curriculum, about JIA, diabetes, otitis media, mastoiditis, and SLE.
As if that wasn’t enough, the questions from this semester’s curriculum were really specific and difficult. I’d paid attention to almost all the seminars and lectures and I found them really difficult.
Everyone was angry after that exam. There was something almost touching about literally everyone coming out from that exam and being like “What the fuck was that shit??”. Almost everyone I’ve talked to have said that it went to shit and that they don’t think they’ll pass. I think I might be able to get a 2.
To rub salt in the wound, they said we wouldn’t get the results back until Tuesday or Wednesday. That’s ridiculous because the first opportunity for the oral B chance is Tuesday, a chance which is completely wasted because no one could sign up for it because we hadn’t had our A chance yet.
Apparently when the Germans had paeds 1 written (which we wanted as well but weren’t allowed to have, we had to have it oral), they needed only 40% to pass. If that’s the case for us as well, it might be okay.
Edit: I don’t know what they ended up to use as the passing limit, but we got our results back this morning and I somehow got a 4. Exam week from hell ended in success 🎉
The exam dates for these four exams this semester lined up perfectly the first exam week to allow for taking all of them in one week. They’re all written exams, so there’s no dignity to be lost in case of a fail, and I’d learned a bit during the semester, so there was a reasonable chance of passing, and I knew I’d probably never need a C chance for them, so the idea was that I had nothing to lose and everything to gain by trying. My plan was to try all of them.
I don’t have much to say about each of them, though.
Pulmonology was the first, at 14:00 on Tuesday. The questions were mostly mediocre, as is standard in POTE written exam. We got the grade at 12 on Thursday. I got a 4 somehow.
Infectology was the second, on Wednesday. Like pulmo, the questions were mostly mediocre, but I somehow got a 4 again. They’d told us that the rules regarding written exams is that the tests have to “quarantine” for 24 hours before correction can start, which is why we’d get our grades in 48 hours. They stayed true to their words, and we got the grade at 12 on Friday.
Medical genetics was the worst of the bunch. It was at 8 on Thursday. Questions about stuff I’d never heard of before, questions I had literally no idea about. I was pretty sure I’d failed, but I somehow got a 3. Funnily enough, the department of genetics didn’t know about the “rule” infecto talked about, and so we got our grades later the same day, Thursday at 12.
The last of these were Endocrinology, which was at 12 on Thursday as well. This was, in my opinion, the least bad of the four. I walked out of there with a pretty good feeling, and got a 4. We got our endo grades at 15:00 on Friday. The head of endocrinology, Emese Mezősi, was present and she made some funny comments and had a relaxed attitude, which is unusual for teachers in higher positions. After reading the rules of the exam out loud, she said “don’t worry guys, the exam is easy”.
All in all it went well grade-wise, but it was very tiring to have to study hard every day with no rest in-between. I know at least four people who followed the same plan (except having public health final on Monday instead of psych, which is an even bigger achievement). It went well but I don’t think I’d recommend this to others.
Psych 2 was my first exam of this semester (excluding family med on Friday week 14, which was easy), and it was the first in a line of 6(!) exams in the first exam week. I’d studied for it with the Anki throughout the whole semester, and I’d reviewed all of it in the 2 days before, so I was pretty well prepared.
It was raining, and I was super nervous ahead of the exam, as before all oral exams (especially the first of the semester). The sound of pouring rain woke me up at 7 and I couldn’t fall back asleep.
I met the other international students and a bunch of Hungarian students under the roof outside the entrance to the Psychiatry department a little before 9. A while after 9, a Hungarian-only speaking secretary comes out and gives us some information (which the Hungarian students there had to translate for us). She then shoots our foreheads with the temperature-gun (which showed 34 degrees for me).
After a while we’re allowed to enter the corridor, and we wait in front of the library of the psychiatry department, where we’re supposed to have our exam. At some point prof. Tenyi arrives and basically repeats the information the secretary gave, and tells us that the exam will be short questions and answers like last semester.
At around 9:45, 45 minutes late, he starts taking in the first students. There were to be two students in the room at the same time, the one who is to be examined and the one next in line. The other student sat inside and waited their turn, and was allowed an opportunity to answer questions the “main” students couldn’t answer.
The Hungarians were the ones to line up first, partly because the information was given in Hungarian first, so the international students were examined after the Hungarians were done.
I was the third international student in line, so I was in the library listening to the second international student’s exam. There was one question they couldn’t answer completely, which was “Which are the two diagnostic criteria for schizo-affective psychosis?”. They couldn’t answer the question, so Tenyi asked me if I knew the answer, but I didn’t. That student got approx 8 – 10 questions, missed only that one question and got a 4.
My turn. Short questions and answers, as usual. I answer all of them well, until he asks one question I was not prepared for. “What’s the name of the self-help group for alcoholics?” My immediate first thought was “Alcoholics anonymous”, which was the correct answer. He then asks “how many steps are there in their program?”, which I had no idea about. Apparently this is something many had learned from TV and stuff, but I didn’t know. I answered that I didn’t know.
He continued asking me questions, all of which I could answer well. I’m pretty sure I got more than 10 questions, more than the previous student, which I thought was because he wanted to give me an opportunity to climb up to the 5. However, after something like 15 questions, he tells me that it’s a 4.
A bit disappointed, seeing as how I was well prepared and that there was only one question which I couldn’t answer, I asked him if we could continue for a 5. He agrees, continues asking 4 – 5 questions, all of which I answer correctly. In the end he gives me the 5.
All in all a nice exam experience, although the stress and anxiety level was high beforeheand. The experience was the same as for psych 1.
I’ve been in a bit of a pickle lately. There are a few topics in the four internal medicine subjects we have this semester which I want to write notes for, but I don’t have time to write all topics in all those subjects, and I don’t want to upload a subject to the website if I’ve only written a few of the topics (looking at you haematology). Haematology really bothers me.
I’ve decided the best way to do this is to jumpstart the notes for internal medicine final in 6th year, seeing as that subject contains the most important topics from all internal medicine sub-specialties. For now, only the pneumonia topic is there, but I plan to write a few more topics in endo, infecto, pulmo, and/or nephro as well. The topics are based on this semester’s lectures, so they should be relevant both for the internal medicine exams this semester as well as for the final on 6th year.
Neurology 2 notes are now up. They’re mostly finished, although there are still some lectures and seminars left and I might make minor changes based on them.
This is the link to this semester’s notes and Anki. The only notes there are neuro 2, and I probably won’t write for any other subjects. The neuro 2 notes are getting close to finished. When they’re almost finished, I’ll upload them to the website like normally, and do the last edits directly on greek.doctor.
For the first time, I’m making Anki flashcards. I’ve made flashcards in these subjects:
Nephrology – based on lectures and seminars
Neurology 2 – based on my notes
Paediatrics 2 – based on questions
Infectology – based on lectures and seminars
Psychiatry (same questions as last semester)
You’re welcome to use them if you want. Every time I add new cards I create a new file in the folder. Download the file and import it, and the new cards will be added to your Anki.
I didn’t do any pranks for april 1st this year, but I wanted to do something fun anyway. Every day greek.doctor receives many spam comments, mostly phishing ones which try to trick you to click a link in the comment. I thought it’d be fun to reply to those comments as if they were real.
Many of the spam comments are obviously targeted for personal blogs and politically motivated ones, which greek.doctor are not, which makes for some funny situations where the comments are very unrelated from the topic they’re commenting on. Some comments are very generic and could fit virtually any personal blog, some try to push medications or vaping, and some push explicit services.
I’ve edited out the phishing information from the comments by replacing them with XXXXX. The topic they’ve commented on is at the top of each picture.