Page created on October 5, 2018. Last updated on December 18, 2024 at 16:56
Normal values of cerebral circulation
The brain needs a very large amount of blood. It weighs only 1300g, approximately 2% of the body weight, but uses 15% of the cardiac output, consumes 25% of the oxygen and 70% of the glucose. There are no energy stores in the neurons, so a short (1-2s) circulatory arrest results in loss of consciousness.
Cerebral blood flow can be measured in absolute terms (700-800 mL/min) or per 100g of brain tissue. On average it is 60 mL/100g/min. If this value decreases below 20 there will be functional abnormalities, and below 10 there are irreversible changes.
Regulation of cerebral circulation
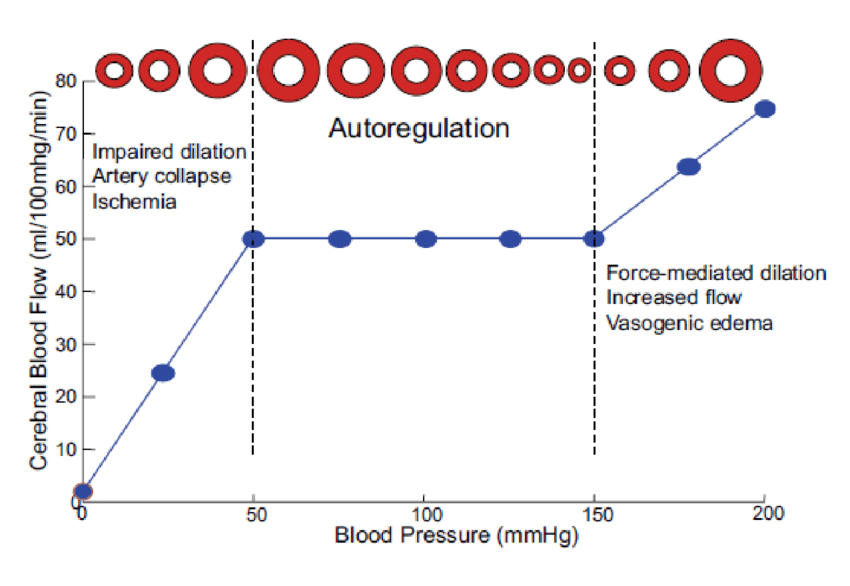
The cerebral blood flow is almost always kept constant, except for epileptic episodes or severe hypotension or hypertension. The cerebral circulation is autoregulated as long as the MAP is between 50 and 150 mmHg and the patient is supine. The brain accomplishes this by the Roy-Sherrington principle, which states that the brain can rearrange the cerebral circulation by controlling vasodilation and vasoconstriction of the vessels. This is how the brain autoregulates its blood flow.
Vasodilation is induced by CO2, low pH, K+, adenosine, NO and a decreased pO2. Vasoconstriction is induced by decreased pCO2 or high pH.
The cerebral autoregulation is impaired when the brain is in a diseased state, like in severe head injury, or ischemic stroke. This leaves the surviving brain tissue unprotected against the effects of blood pressure changes. The regulation is also lost in the tissue surrounding a space-occupying brain lesion like a tumour or a hematoma.
In chronic hypertension the range where CBF is autoregulated is shifted upwards (like e.g. towards 100 – 200 mmHg instead of the normal 50 – 150). If these patients suddenly decrease their MAP to normal values (around 90 mmHg) they will experience cerebral hypoperfusion.
The cerebral blood flow as a whole is constant. However the blood flow can be redirected to different parts of the brain depending on the need. As an example will Broca’s area receive more blood flow during talking.
Does the Roy-Sherrington principle explain how the cerebral blood flow is redirected to active brain tissue, or does it explain how the cerebral blood flow is autoregulated?
Can you clarify? 🙂
The latter. I’ve added a sentence about it to clarify.
The classical theory was that cerebral blood flow is redirected to active neurons because active neurons have higher metabolism, which increases the level of metabolic byproducts like CO2 and adenosine, which in turn vasodilates nearby vessels.
However, the local blood flow increases more than their metabolic activity would indicate, so that doesn’t appear to be the whole picture. You can read more in this article. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3206737/