Table of Contents
Page created on April 23, 2020. Last updated on May 24, 2022 at 09:40
General knowledge
- The cardiology topics I’ve written for the internal medicine final are much better than these, and are based on the lectures. I recommend using those primarily to study for cardiology. They cover most of the topics.
- The most important topics for the exam are those related to atrial fibrillation, ACS, and heart failure
- Upper year students recommend reading through the handout the department of cardiology have written, and to do the sample questions in it
- History taking in cardiology
- Fever?
- Myocarditis, pericarditis, endocarditis
- Orthopnoea?
- Patient can’t breathe when lying down because they depend on the accessory breathing muscles to breathe
- Palpitations?
- What makes them start?
- Is the heart rate irregular during the palpitations?
- Is the heart rate fast during the palpitations?
- Does the heart skip beats during the palpitations?
- Have you experienced syncope?
- Fever?
- Physical examination in cardiology
- Inspection
- Varicose veins
- Jaundice
- Pallor
- Cyanosis
- Clubbing
- “Mitral face”
- Rosy cheeks but rest of face is cyanotic
- Seen in severe mitral stenosis
- Osler nodes
- Painful subcutaneous nodules on fingers, toes
- Indicates infective endocarditis
- Janeway lesions
- Non-painful, erythematous macules on palms, soles
- Indicates infective endocarditis
- Medial sternotomy scar
- Indicates previous bypass operation (CABG)
- Saphenectomy scar
- Indicates previous CABG
- Marfan syndrome
- Kyphoscoliosis
- Barrel chest
- Pectus excavatum
- Distended jugular vein
- Indicated right heart failure
- Cardiac cachexia
- Palpation
- Pulsus alternans
- Alternating weak and strong peripheral pulse
- Seen in HF
- Pulsus parvus
- Weak pulse
- Pulsus tardus
- Delayed pulse
- Pulsus alternans
- Auscultation
- Describe heart sounds:
- Frequency
- Rhythmic or not
- Description of the murmur
- Thrill = palpable murmur
- Midsystolic = murmur which beings after S1 and ends before S2
- Holosystolic = murmur heard throughout the whole systole
- Continuous murmur = murmur heard throughout systole and diastole
- Grade I – murmur just barely hearable
- Grade II – murmur is faint but immediately hearable
- Grade III – easily hearable, but no thrill
- Grade IV – loud murmur with thrill
- Grade V – loud murmur with thrill. Hearable with just the rim of the stethoscope touching the chest
- Grade VI – loud murmur with thrill. Hearable with the stethoscope above the chest
- Pericardial rub
- Describe heart sounds:
- Inspection
1. Basic principles of ECG analysis
2. Special cardiological investigations I: Stress tests, Holter monitoring and Ambulatory Blood Pressure Monitoring (ABPM)
- Exercise ECG
- Safety precautions
- There is a small (1:10 000) risk of sudden cardiac death
- Doctor and resuscitation equipment must be available
- Test may be performed on treadmill or bicycle
- Test follows the Bruce protocol, which determines when and how much the treadmill speed and incline increases
- Patient is equipped with 12-lead ECG which monitors heart during and after exercise
- Indications
- To diagnose chronic coronary syndrome
- To evaluate progression of chronic coronary syndrome
- Contraindications
- Recent acute myocardial infarction
- Ongoing unstable angina
- Active endocarditis
- Decompensated heart failure
- Signs of myocardial ischaemia of ECG
- ST depression > 1 mm in anterior leads
- ST depression > 2 mm in inferior leads
- Reasons of exercise termination
- Test should ideally continue until the patient feels that they cannot exercise further
- Determined by the patient
- If the patient requests to stop and they experience significant symptoms (like angina, dyspnoea, etc.)
- If the patient requests to stop but is not experiencing significant symptoms, the patient should be encouraged to continue
- Determined by the result of the ECG
- ST depression
- BBB
- High grade AV block
- Ventricular arrhythmias
- Duke treadmill score
- Scores the patient based on three parameters
- Exercise time
- Maximum ST segment deviation
- Presence of angina
- The higher the Duke score the higher the risk for complicated CAD
- Scores the patient based on three parameters
- Sensitivity, specificity, diagnostic accuracy
- 45 – 60% sensitive
- 70 – 90% specific
- If the patient can’t reach at least 85% of the max heart rate the sensitivity of the test decreases
- Pharmacological stress
- For patients who cannot exercise, drugs can be used to induce stress
- Dobutamine
- Dipyridamole
- Safety precautions
- Other stress tests
- Echocardiography, nuclear imaging and MRI may all be performed under stress to reveal ischaemic changes
- These tests have much higher sensitivity than exercise ECG
- Holter ECG
- 24 hour or longer continuous ECG monitoring
- Different types have different number of leads
- Most have between 3 and 8 leads
- A small, lightweight recorder is connected to electrodes placed on the patient’s chest and continuously record the ECG
- The patient can be home during this period
- Afterwards the doctor can read the recordings
- Indications for Holter ECG
- Detection of intermittent arrhythmias which may not be present on office ECG
- Detection of ischaemia
- 24 hour or longer continuous ECG monitoring
- Ambulatory blood pressure monitoring
- Patient wears a device which measures blood pressure and heart rate over a 24 – 48-hour period
- Several parameters are recorded
- Heart rate
- Minimum blood pressure
- Maximum blood pressure
- Average blood pressure
- Diurnal index
- The difference between daytime and night-time mean blood pressure
- Blood pressure at night should normally be more than 10 lower than blood pressure at daytime
- Those who have diurnal index < 10 % are called “non-dippers”
- Those who have diurnal index > 10 % (normal) are called “dippers”
- Hypertensive time index
- The percentage of time where the BP was higher than normal
- Should be lower than 25 %
3. Special cardiological investigations II: Echocardiography, nuclear methods, computed tomography, cardiac MRI
- Echocardiography
- Best tool to diagnose organic heart disease
- Can be performed in rest or with exercise or pharmacological stress
- Can be performed outside the chest (transthoracic echo, TTE) or from inside the oesophagus (transoesophageal echo, TEE)
- Indications
- Valve abnormalities
- Evaluation of myocardial contractility
- Septal defects
- Aneurysms
- Thrombi
- Vegetations
- Nuclear cardiology
- Myocardial perfusion studies
- Can detect abnormalities of myocardial perfusion
- Shows regional distribution of myocardial perfusion
- Uses a radiopharmaceutical which accumulates in myocardium proportionally to the regional myocardial blood flow
- Uses either SPECT or PET
- Can be performed in rest or with exercise or pharmacological stress
- Findings
- Normal
- Homogeneous uptake of the radiopharmaceutical throughout the myocardium
- Defect (infarct)
- A localized area of myocardium with less radiopharmaceutical uptake than the rest
- Reversible defect (ischaemia)
- A localized area of myocardium with less radiopharmaceutical uptake than the rest
- Uptake normalizes during rest
- Normal
- Radionuclide ventriculography
- Evaluates left ventricular function
- Uses a radiopharmaceutical which accumulates in blood, showing the movement of blood through the heart and therefore the left ventricular function
- Myocardial perfusion studies
- Cardiac CT
- Better than MRI in the evaluation of the coronaries
- Is usually ECG-gated, to synchronize the scan sequence to the patient’s heartbeat
- This improves image quality and reduces the radiation dose
- Non-contrast cardiac CT
- Used to determine coronary artery calcium score (CAC) score
- The CAC score is based on the area of calcified atherosclerosis in the coronaries
- Used in risk stratification of CAD patients
- Contrast cardiac CT (= Coronary CT angiography)
- Used in the diagnosis of CAD
- Cardiac MRI (= cardiovascular magnetic resonance (CMR))
- Better than CT in the evaluation of the cardiac anatomy and function
- Is usually ECG-gated, to synchronize the scan sequence to the patient’s heartbeat
- This improves image quality
- CMR is the gold standard for LV and RV size and function
- Special types
- Stress perfusion MRI
- Adenosine is given to simulate exercise
- The myocardial perfusion can then be determined
- Viability MRI
- Can determine areas of myocardium which are viable or infarcted
- CMR is the gold standard for evaluation of viability
- Viable myocardium can recover its contractility upon revascularization
- If there is viable myocardium, revascularization will improve contractility
- Stress perfusion MRI
4. Special cardiological investigations III: Invasive studies (electrophysiology, heart catheterization, coronary angiography, and coronary interventions)
- Cardiac catheterization
- Refers to any procedure where a catheter is inserted into a peripheral vessel and led back to the heart
- Can be used for both diagnostic and therapeutic procedures
- Diagnostic procedures
- Cardiac electrophysiology
- Right heart catheterization
- Coronary angiography
- Therapeutic procedures
- Percutaneous coronary intervention (PCI)
- Diagnostic procedures
- The catheters are often radiopaque, so they’re visible on x-rays
- Fluoroscopy is often used to visualize the catheters as they’re guided to their target position
- Invasive cardiac electrophysiology studies
- Allows analysis of arrhythmias and treatment of them
- Indications
- Arrhythmias who are not sufficiently treated by medication
- WPW syndrome
- AVNRT
- Atrial fibrillation
- Atrial flutter
- Ventricular tachycardia
- Procedure
- Catheter is inserted into patient’s femoral vein
- The catheter is led to the point of interest in the right heart
- The catheter can measure intracardiac ECGs along the conduction system of the heart
- Recordings are often acquired from the high right atrium (SA node), tricuspid annulus (His bundle), and right ventricular apex
- The catheter can also pace the heart from the inside, allowing for examination of the conduction system and how the impulses propagate in the heart
- Cardiac mapping is performed, where they look for the area which must be treated to cure the arrhythmia
- After the area of interest has been determined, the catheter can ablate the area by burning or freezing it, thereby killing the abnormal myocardial cells, hopefully treating the arrhythmia
- Mapping can be performed again after ablation, to determine whether the ablation was successful
- If not, more ablation may be necessary
- Right heart catheterization (= pulmonary artery catheterization)
- A catheter which can measure pressures is led into the right heart and the pulmonary artery
- Right heart catheterization can provide may useful parameters
- Central venous pressure
- Right atrial pressure
- Right ventricular pressure
- Pulmonary arterial pressure
- Pulmonary capillary wedge pressure (PCWP)
- The PCWP is equal to the left atrial pressure
- Cardiac output
- Venous oxygen saturation
- Indications
- Differentiation among causes of shock
- Differentiation between mechanisms of pulmonary oedema
- Evaluation of pulmonary hypertension
- Procedure
- A Swan-Ganz catheter is inserted into the right jugular vein and led into the right heart
- The catheter has an inflatable balloon at its tip
- The catheter is advanced into the left pulmonary artery
- The balloon on the catheter is inflated inside the pulmonary artery, causing it to become wedged
- A Swan-Ganz catheter is inserted into the right jugular vein and led into the right heart
- Coronary angiography
- A catheter from which contrast material can be ejected is inserted into a peripheral artery and led back to and into the coronary arteries
- Therapeutic procedures (PCI) can be performed in the same setting, if the findings of the angiography warrant it
- Indications
- Evaluation of coronary artery disease
- Procedure
- Catheter is inserted into radial (recommended) or femoral artery
- Catheter is led back to the aortic sinus
- Catheter is led into the orifice for the coronary artery to be examined
- Contrast is ejected out of the catheter, which allows visualization of the coronary artery, its branches and any obstructions
- Percutaneous coronary intervention (PCI)
- See topic 17
General about arrhythmias
- Arrhythmias can be classified as tachyarrhythmias or bradyarrhythmias
- They can be further classified according to their site of origin
- Tachyarrhythmias can also be classified according to the morphology of the QRS complex
- Bradyarrhythmias (< 60 bpm)
- Bradyarrhythmias of SA nodal or atrial origin
- Respiratory sinus arrhythmia
- Sinus bradycardia
- Sick sinus syndrome
- Bradyarrhythmias of AV nodal origin
- First degree AV block
- Second degree AV block
- Third degree AV block
- Bradyarrhythmias of SA nodal or atrial origin
- Tachyarrhythmias (> 100 bpm)
- Supraventricular tachyarrhythmias
- Supraventricular premature beats
- Sinus tachycardia
- Atrial flutter
- Atrial fibrillation
- Atrial tachycardia
- AV reentry tachycardia (AVRT)
- AV nodal reentry tachycardia (AVNRT)
- Junctional tachycardia
- Ventricular tachyarrhythmias
- Premature ventricular beats
- Ventricular tachycardia
- Torsade de pointes
- Ventricular fibrillation
- Tachyarrhythmias with narrow (normal) QRS
- Atrial fibrillation
- Atrial flutter
- Orthodromic AV reentry tachycardia (AVRT)
- AV nodal reentry tachycardia (AVNRT)
- Tachyarrhythmias with wide QRS
- Ventricular fibrillation
- Ventricular flutter
- Ventricular tachycardia
- Antidromic AV reentry tachycardia (AVRT)
- Supraventricular tachyarrhythmias
5. Mechanisms of arrhythmias
- Three major mechanisms underlie tachyarrhythmias
- Many tachyarrhythmias involve more than one of these mechanisms
- Some tachyarrhythmias have unknown exact underlying mechanism, like AF and VF, but it is assumed that they are the result of a combination of multiple mechanisms
- Reentry
- Normally the cardiac cycle begins when an impulse leaves the SA node. The impulse dies out when all fibres have been depolarized and are in the refractory period
- If, for some reason, there are always some fibres which are not in the refractory period, the impulse will never die and instead form a small reentry circuit
- The reentry circuit will rapidly conduct impulses to the surrounding myocardium
- Macro-reentry – refers to large reentry circuits
- Atrial flutter
- AVRT
- Micro-reentry – refers to small reentry circuits
- AVNRT
- Monomorphic ventricular tachycardia
- Enhanced or abnormal automaticity
- Enhanced automaticity = pacemaker cells spontaneously depolarize more frequently than normal
- Abnormal automaticity = non-pacemaker cells acquire automaticity, allowing them to depolarize spontaneously
- Hypoxic causes depolarization of cells, so ischaemia is a common cause of abnormal automaticity and therefore tachyarrhythmias
- Triggered activity
- Refers to abnormal depolarization of pacemaker cells which occur during or after the repolarization phase of a normal action potential
- The result is that a normal impulse is quickly followed by an abnormal impulse
- This can cause extrasystoles, which can precipitate other tachyarrhythmias via the other mechanisms
- Early afterdepolarization (EAD)
- Abnormal depolarization which occurs during the repolarization phase of a normal action potential
- Delayed afterdepolarization (DAD)
- Abnormal depolarization which occurs after the repolarization phase of a normal action potential
- Refers to abnormal depolarization of pacemaker cells which occur during or after the repolarization phase of a normal action potential
- Two major mechanisms underlie bradyarrhythmias
- Decreased automaticity
- Conduction blocks
- UpToDate has a good article on this here, and another good article is here
6. Sinus and atrial arrhythmias
- Sinus arrhythmias
- Sinus bradycardia
- Sinus tachycardia
- Sick sinus syndrome
- Atrial arrhythmias
- Atrial premature beats
- Atrial tachycardia
- Atrial fibrillation
- Atrial flutter
- Sick sinus syndrome (= sinus node dysfunction) (SSS or SND)
- Refers to any dysfunction of the SA node
- Often due to idiopathic degeneration and fibrosis of the SA node
- Can also be due to drug side effects or ischaemia
- Results in abnormal automaticity and/or intranodal conduction
- It’s a progressive disease, so symptoms become worse and worse over time
- As the degeneration starts to affect the entire right atrium, atrial arrhythmias may occur
- Patients usually experience periods of normal SA node function, interrupted by symptomatic periods
- Over time symptoms become worse and occur more and more often
- Clinical features
- Light-headedness
- Presyncope
- Syncope
- Palpitations
- Possible ECG manifestations
- Early
- Sinus bradycardia
- Sinus arrests
- SA block
- Inadequate heart rate increase in response to activity
- Late (after progressing, and the atria have become affected)
- Atrial fibrillation
- Atrial flutter
- Tachycardia-bradycardia syndrome
- Early
- Tachycardia-bradycardia (tachy-brady) syndrome
- Tachy-brady syndrome occurs in 50% of patients with SSS
- It refers to the presence of episodes where sinus bradycardia and atrial tachycardia (often atrial fibrillation) alternate
- Treatment
- If caused by drug side effects or ischaemia: treatment of underlying cause
- Permanent pacemaker
- Anticoagulation
- If atrial fibrillation or flutter is present
- Refers to any dysfunction of the SA node
- Atrial fibrillation (AF, Afib)
- The most common sustained arrhythmia
- Epidemiology
- 3% of adults (20 or older)
- Prevalence is higher in older persons
- Etiology
- No direct cause of AF is known, but many risk factors are known
- Old age
- 95% of patients are over 60
- Hypertension
- Coronary artery disease
- Alcohol
- Heart failure
- Valvular heart disease
- Hyperthyroidism
- Cardiac surgery
- Pathophysiology
- Multiple mechanisms can contribute to atrial fibrillation
- Volume overload -> atrial remodelling
- Atrial ischaemia
- Inflammation of atrium
- AF is initiated by an ectopic focus, often near the pulmonary veins or in fibrotic atrial tissue
- AF is sustained by micro-reentry or by rapid firing from the ectopic focus
- Fibrillation of the atria causes remodelling of the atrial myocardium, creating an evil cycle
- Atrial fibrillation causes stasis of the blood in the atria, increasing risk for thromboembolism
- During AF the atria contract hundreds of times per minute, but the AV node prevents most of these impulses from conducting to the ventricles
- However, many impulses will be conducted, which results in a ventricular heart rate of > 100
- If an accessory atrioventricular pathway exists, the impulses from the atria can bypass the AV node and cause FBI arrhythmia (see topic 8)
- Multiple mechanisms can contribute to atrial fibrillation
- Types of AF according to timescale
- Paroxysmal AF
- AF starts and stops by itself
- Persistent AF
- AF that has persisted for than 7 days without stopping by itself
- Long-standing persistent AF
- AF that has persisted for than 1 year without stopping by itself
- Permanent AF
- AF which will not stop by itself, and the patient and clinician has decided to no longer try to restore sinus rhythm
- Paroxysmal AF
- Types of AF according to etiology
- Valvular AF
- AF which occurs in patients with mitral stenosis or artificial valves
- Has higher risk of stroke than non-valvular AF
- Non-valvular AF
- All other cases
- Valvular AF
- Clinical features
- Many are asymptomatic
- Symptoms may be precipitated by exercise, emotion, alcohol, etc.
- Absolutely irregular pulse
- Palpitation
- Dizziness
- Syncope
- Diagnosis
- ECG
- Absolutely irregular RR intervals +
- Absence of P waves
- Tests to look for other heart diseases
- Echocardiography
- TSH level
- ECG
- CHA2DS2-VASc score
- This score system estimates the patient’s annual risk for thromboembolism due to AF
- Each letter is an acronym for a risk factor
- The presence of the risk factors gives one point
- Exception is the presence of those letters which are followed by a 2 (like A2), which give two points
- C – chronic heart failure
- H – hypertension
- A2 – Age > 75
- D – Diabetes
- S2 – Previous stroke, TIA or thromboembolism
- V – Cardiovascular disease
- A – Age 65 – 74
- Sc – Sex category
- Female sex gives 1 point
- Male sex gives 0 points
- Annual stroke risk based on score
- Score 0 – risk 0%
- Score 1 – risk 1%
- Score 2 – risk 2%
- Score >6 – risk >9%
- HAS-BLED score
- This score system estimates the annual risk of major bleeding in patients taking anticoagulation for atrial fibrillation
- Each letter is an acronym for a risk factor
- The presence of the risk factors gives one point
- H – Hypertension
- A – Abnormal renal function or abnormal liver function
- 1 point for each
- S – Previous stroke
- B – Previous major bleeding
- L – Labile (too high) INR
- E – Elderly (age > 65)
- D – Drugs which predispose to bleeding or alcohol abuse
- 1 point for each
- Drugs like NSAIDs, antiplatelets
- A score of 3 or higher can be considered “high”
- For all patients with CHA2DS2-VASc score 2 or higher, the benefits of anticoagulation far outweigh the risks of bleeding, no matter the HAS-BLED score
- For this reason, the HAS-BLED score should NOT be weighed against the CHA2DS2-VASc score to decide whether the patient should be anticoagulated
- Instead, HAS-BLED is used to identify potentially reversible risk factors which can be treated, and to give the patient and physician insight to the bleeding risk
- Treatment
- Treatment revolves around two parts: preventing embolization and stroke, and reducing symptoms by rate control or rhythm control
- Both rate and rhythm control reduce symptoms, but each have their advantages and drawbacks
- In general, those who have significant symptoms should try rhythm control, while other patients should try rate control
- A patient can’t be both rate and rhythm controlled
- Cardioversion
- Refers to converting AF to sinus rhythm
- Pharmacological cardioversion may take anywhere from 30 minutes to hours after the IV administration of the drug
- Cardioversion in case of haemodynamic instability
- Should be done by electrical cardioversion
- Cardioversion in case of haemodynamic stability
- Can be done by electrical or pharmacological cardioversion
- Class Ic antiarrhythmics or vernakalant
- Amiodarone
- If the patient has ischaemic or structural heart disease, or heart failure
- Before cardioversion, it’s important to be sure that there is no thrombus in the left atrial appendage
- If the AF is not new (within 48 hours) and the patient wasn’t anticoagulated, transesophageal echocardiography must be performed first to ensure there is no thrombus
- If there is a thrombus, cardioversion can loosen it, causing embolization
- Prevention of embolization by oral anticoagulation
- In all patients with CHA2DS2-VASc score 2 or more
- If the score is 1, clinical judgement and HAS-BLED score should decide whether anticoagulation provides benefits which outweigh the risks
- If the score is 0 oral anticoagulation is contraindicated
- In all patients with moderate or severe mitral stenosis, regardless of CHA2DS2-VASc score
- Anticoagulation by NOACs or VKAs (INR 2 – 3)
- NOACs are contraindicated in valvular AF
- In all patients with CHA2DS2-VASc score 2 or more
- (Heart) rate control
- Refers to using medications to reduce the resting (ventricular) heart rate to < 110 bpm
- No effort is made to maintain sinus rhythm
- Class II or class IV antiarrhythmic or digoxin may be used
- Rate control and rhythm control both have the same survival prognosis, only symptoms are different
- Rhythm control
- Refers to maintaining sinus rhythm, and preventing conversion to AF
- Can be done pharmacologically or by ablation
- Class III or class Ic antiarrhythmics may be used
- “Pill-in-the-pocket” approach
- For some patients who are easily pharmacologically cardioverted and only have symptoms infrequently (like once a month or even less frequently)
- They may carry an oral dose of an antiarrhythmic, and take it whenever they have symptoms to cardiovert themselves
- Flecainide or propafenone (class Ic drugs) may be used
- Catheter ablation
- Atrial fibrillation is often triggered by ectopic foci close to the pulmonary veins
- Catheter ablation can electrically isolate the pulmonary veins, preventing impulses from being conducted from there to the rest of the atria
- Catheter ablation can be performed if antiarrhythmic drugs fail, or as first-line therapy in some patients with symptomatic paroxysmal AF
- Treatment revolves around two parts: preventing embolization and stroke, and reducing symptoms by rate control or rhythm control
- Complications
- Tachycardia-induced cardiomyopathy
- Stroke
- Atrial flutter
- Very similar to atrial fibrillation in clinical appearance
- Differences from atrial fibrillation
- The pulse is regular rather than irregular
- The ECG shows F waves instead of P waves
- Is due to a macro-reentry rather than a micro-reentry
- Many cases of atrial flutter eventually degenerate into AF
- Clinical features and treatment are similar as in AF
7. Arrhythmias involving the AV node and accessory pathways
- Paroxysmal supraventricular tachycardia (PSVT)
- Refers to supraventricular tachycardias who start and stop suddenly
- Three underlying diseases can cause PSVT
- AVNRT
- AVRT
- Paroxysmal atrial tachycardia
- Clinical features
- Like the arrhythmia itself, the symptoms stop and start suddenly
- Palpitations
- Dizziness
- Dyspnoea
- Treatment
- For acute termination of PSVT
- For haemodynamically unstable patients: Electrical cardioversion
- Vagal manoeuvres
- These manoeuvres increase parasympathetic tone, which may suddenly terminate the PSVT
- They should always be tried before medical therapy
- Valsalva manoeuvre
- Carotid sinus massage
- Medical treatment
- Depends on the underlying condition
- For long-term prevention of PSVT
- For many patients, simply instructing them to perform vagal manoeuvres any time they experience symptoms is enough
- For those patients where vagal manoeuvres aren’t enough, catheter ablation of the accessory pathway is recommended
- For acute termination of PSVT
- AV nodal reentry tachycardia (AVNRT)
- Accounts for 60% of cases of PSVT
- AVNRT is characterised by the paroxysmal formation of a micro-reentry circuit within the AV node
- Pathophysiology
- The AV node contains two electrical pathways, which paroxysmally form a reentry circuit
- This circuit continuously conducts impulses to the ventricles, causing tachycardia
- Treatment
- To stop PSVT if vagal manoeuvre failed: Adenosine
- Curative treatment: Catheter ablation of accessory pathway in the AV node
- AV reentry tachycardia (AVRT)
- Accounts for 30% of cases of PSVT
- AVRT is characterised by the paroxysmal formation of a macro-reentry circuit across the AV node and an accessory fibre
- The most common cause of AVRT is the presence of the bundle of Kent, which characterizes Wolff-Parkinson-White syndrome
- WPW syndrome is the most common cause of AVRT
- Pathophysiology
- The heart contains an accessory pathway which connects the atria and ventricles
- The accessory pathway paroxysmally forms a macro-reentry circuit with the AV node
- This circuit continuously conducts impulses to the ventricles, causing tachycardia
- Depending on whether the antegrade conduction passes through the AV node or the accessory fibre AVRT can be classified as orthodromic or antidromic
- Orthodromic AVRT
- Accounts for 95% of cases of AVRT
- The impulse passes from the atria to the ventricles through the AV node, and then back to the atria through the accessory pathway
- Diagnosis
- P wave after QRS
- Narrow QRS complex
- No delta wave!
- Delta wave is only present in antidromic AVRT
- This means that only a few WPW patients have delta waves during AVRT
- All WPW have delta-waves during rest, however
- Treatment
- To stop PSVT if vagal manoeuvre failed: Adenosine
- Curative treatment: Catheter ablation of accessory pathway
- Antidromic AVRT
- Accounts for only 5% of cases of AVRT
- The impulse passes from the atria to the ventricles through the accessory pathway, and then back to the atria through the AV node
- Unlike the AV node, the accessory pathway doesn’t delay the conduction
- This is what causes the pre-excitation of the ventricles, which causes the characteristic delta wave
- Diagnosis
- Delta wave on QRS complex (causes the QRS complex to be wide)
- Treatment
- To stop PSVT if vagal manoeuvre failed: Procainamide
- AV node-blocking drugs (adenosine, class II, III, IV) must never be given to patients with antidromic AVRT as they can cause ventricular tachycardia
- Curative treatment: Catheter ablation of accessory pathway
- To stop PSVT if vagal manoeuvre failed: Procainamide
8. Ventricular arrhythmias
- All ventricular arrhythmias have wide QRS
- Ventricular premature beats
- Also called premature ventricular contractions (PVC) and ventricular extrasystoles (VES)
- Up to 80% of healthy people may have occasional asymptomatic VES
- Etiology
- Virtually any heart disease
- COPD
- Virtually any endocrinological disease
- Virtually any stimulating drug, nicotine or alcohol
- Interestingly, caffeine has not been shown to increase the risk of VES
- Classifications
- According to etiology
- Idiopathic VES
- VES in the presence of heart disease
- According to origin and morphology
- Unifocal (monomorphic) or multifocal (polymorphic)
- Depending on whether they originate from one or multiple sites in the ventricles
- Unifocal (monomorphic) or multifocal (polymorphic)
- According to etiology
- Special types
- Ventricular bigeminy – every normal beat is followed by a VES
- Ventricular trigeminy – two normal beats are followed by a VES
- Couplets – two VES in a row
- Triplets – three VES in a row
- Clinical features
- The vast majority are asymptomatic
- Palpitation
- Dizziness
- Diagnosis
- No preceding P wave
- Wide QRS
- Abnormal QRS morphology
- Multifocal extrasystoles may have different QRS morphology, as they originate from different sites in the ventricles
- T wave points in the opposite direction of QRS
- A full compensatory pause is present after the VES
- Treatment
- No treatment is needed in most cases
- Beta blockers or CCBs are the first line
- Catheter ablation can be used if antiarrhythmics fail
- Ventricular tachycardia (VT, V-tach)
- Defined as three or more consecutive QRS complexes at a rate > 100 bpm
- Etiology
- Idiopathic
- Idiopathic VT often has a good prognosis
- Cardiomyopathies
- Ischaemic heart disease
- Myocardial infarction
- Both in the acute and chronic phase
- Myocardial infarction
- Long QT syndrome
- Idiopathic
- Classification
- According to timeline
- Nonsustained VT – lasts less than 30 seconds
- Sustained VT – lasts more than 30 seconds OR is terminated within 30 seconds due to haemodynamic compromise
- According to morphology
- Monomorphic ventricular tachycardia – all QRS complexes are identical
- Polymorphic ventricular tachycardia – the QRS complexes are not identical
- According to timeline
- Pathophysiology
- The combination of rapid ventricular rate and atrioventricular dissociation may decrease CO
- Clinical features
- Often asymptomatic, especially if nonsustained
- Palpitations
- Syncope
- Haemodynamic instability
- Cardiogenic shock
- Cardiac death
- Torsade de pointes
- A form of polymorphic ventricular tachycardia which occurs due to an extrasystole on a prolonged QT
- The ECG morphology appears to “twist” around the isoelectric line
- Hence the name, which means “twisting of the points”
- It often terminates suddenly, but it can degenerate into VF and is therefore and emergency
- Treatment
- In haemodynamically unstable patients: Electrical defibrillation
- In haemodynamically stable patients
- IV magnesium sulphate – both terminates and prevents it short-term
- Treatment
- If haemodynamically unstable:
- With pulse -> cardioversion
- Without pulse -> defibrillation
- If haemodynamically stable:
- Antiarrhythmics
- Treat any underlying cause
- If haemodynamically unstable:
- Prevention
- By ICD implantation
- See topic 10 and surgery 1 topic 25
- Ventricular fibrillation (VF. V-fib)
- Defined as rapid (> 300 bpm), absolutely irregular ventricular rhythm with variable QRS morphology
- Etiology
- Ischaemic heart disease
- Especially myocardial infarction
- Myocarditis
- Cardiomyopathy
- WPW syndrome
- Long QT
- Long QT can either directly cause VF or first cause torsade, which will degenerate into VF
- Ischaemic heart disease
- Pathophysiology
- Fibrillation of the ventricles means that there are no haemodynamically effective contractions in the ventricles, causing severely decreased CO
- Unlike VT, VF will not terminate by itself
- Clinical features
- Never asymptomatic
- Early symptoms are nonspecific
- Chest pain
- Palpitations
- Dyspnoea
- Dizziness
- Late symptoms:
- Loss of consciousness
- Cardiac death
- Treatment
- Defibrillation
- Necessary to prevent death
- Treat underlying cause
- Defibrillation
- Prevention
- By ICD implantation
- See topic 10 and surgery 1 topic 25
9. AV blocks and ventricular conduction defects
- AV blocks
- Etiology
- Ischaemic heart disease
- Especially myocardial infarction
- Cardiomyopathies
- Myocarditis
- Electrolyte disturbances
- AV-blocking drugs
- Digoxin
- Beta blockers
- CCBs
- Cardiac surgery and other cardiac procedures
- Ischaemic heart disease
- Treatment
- If haemodynamically unstable
- Atropine
- It increases conduction through the AV node
- Temporary pacing of the heart
- Transcutaneous or transvenous pacing (see surgery 1 topic 25)
- Atropine
- If haemodynamically stable
- Look for and treat underlying reversible causes
- If AV block remains -> permanent pacemaker
- If haemodynamically unstable
- 1st degree AV block
- Often asymptomatic and benign
- PQ interval > 200 ms
- Needs no treatment
- 2nd degree AV block – Mobitz type I (Wenkebach)
- Often as a side effect of AV-blocking drugs
- Progressive lengthening of PQ interval until one beat is dropped
- Usually asymptomatic
- 2nd degree AV block – Mobitz type II
- Some P waves are not conducted to the ventricles
- Every second P wave is conducted (2:1 block)
- Every third P wave is conducted (3:1 block)
- Out of three P waves, 2 are conducted (3:2 block)
- Rarely asymptomatic
- Fatigue
- Dizziness
- Presyncope/syncope
- Often degenerates into 3rd degree AV block
- Some P waves are not conducted to the ventricles
- 3rd degree AV block (= complete heart block)
- Almost never asymptomatic
- Symptoms depend on the escape rhythm
- Most escape rhythms are 40 bpm or less, which produces insufficient CO, causing symptoms like fatigue, chest pain, presyncope/syncope
- If the patient has escape rhythm of 50 or more (rare), they might be asymptomatic
- If no escape rhythm sets in (rare), sudden cardiac death will occur
- Escape rhythms are often unstable, so patient must be closely monitored until they can be paced
- High grade AV block refers to either Mobitz type II or complete heart block
- Etiology
- Intraventricular conduction defects
- Etiology
- Ischaemic heart disease
- Especially myocardial infarction
- Heart failure
- Pulmonary embolism
- Myocarditis
- Ischaemic heart disease
- These conditions, when present without any other heart disease, are asymptomatic and don’t require any treatment
- However, because they’re often found in the context of heart disease the patient should be examined for heart disease if an intraventricular conduction defect is found
- Right bundle branch block (RBBB)
- Refers to a block within the right bundle branch
- This block delays the conduction of the right ventricle, because the right ventricle must be depolarized through the ventricular myocardium from the left ventricle after the left ventricle has been depolarized normally
- rSR’ (rabbit ears) in leads V1, V2
- The 2nd R-wave in the rabbit ears is the result of the delayed depolarization of the right ventricle
- Leads V1, V2 correspond to the right ventricle
- Wide S in leads I, aVL, V5, V6
- Wide QRS
- Due to the delayed depolarization of the right ventricle
- Left bundle branch block (LBBB)
- Refers to a block within the left bundle branch
- This block delays the conduction of the left ventricle, because the left ventricle must be depolarized through the ventricular myocardium from the right ventricle after the right ventricle has been depolarized normally
- Wide, notched R wave (“M”-pattern) in leads I, aVL, V5, V6
- Leads I, aVL, V5, V6 correspond to the left ventricle
- Deep S in leads V1, V2
- Wide QRS
- Due to the delayed depolarization of the left ventricle
- New onset LBBB can indicate acute myocardial infarction
- Left anterior fascicular block (= left anterior hemiblock)
- Narrow QRS
- Left axis deviation (-45 to -90 degrees)
- Left posterior fascicular block (= left posterior hemiblock)
- Narrow QRS
- Right axis deviation (90 – 180 degrees)
- Etiology
10. Syncope and sudden cardiac death
- Syncope
- Syncope refers to the transient loss of consciousness due to cerebral ischaemia
- It is self-limiting by definition, and rarely lasts more than a minute
- Etiology
- Vasovagal syncope
- Orthostatic hypotension
- Large pulmonary embolism
- Cardiac syncope
- High grade AV block
- Sick sinus syndrome/sinus node dysfunction
- Ventricular fibrillation
- Ventricular tachycardia
- Aortic stenosis
- If severe
- Hypertrophic cardiomyopathy
- If the left ventricular outflow tract is obstructed, or due to arrhythmias
- Atrial myxoma
- The myxoma may obstruct the mitral or tricuspid valve
- Pericardial tamponade
- Aortic dissection
- Many of the conditions causing syncope can also cause sudden cardiac death
- Patients experiencing syncope must be examined for the underlying cause, and measures to prevent sudden cardiac death may be necessary
- Cardiac syncope is associated with a 40% risk of sudden cardiac death within 1 year
- Diagnosis
- ECG
- Holter ECG may prove very useful
- Echocardiography
- ECG
- Adams-Stokes syndrome
- A syndrome characterised by episodes of syncope (Adams-Stokes “attacks”)
- Classically referred to syncope due to 3rd degree AV block
- Nowadays refers to syncope due to any cardiac arrhythmia
- Sudden cardiac death (SCD)
- Cardiac arrest refers to a sudden, unexpected cessation of cardiac activity, causing haemodynamic collapse
- “Sudden” means occurring within an hour of onset of symptoms, if the patient was symptomatic
- If the patient didn’t recently have cardiovascular symptoms, “sudden” means occurring within 24 hours of when the patient was last seen without symptoms
- If the patient is not treated in time, death occurs, in which case the incidence is called sudden cardiac death
- Of course, the cause of death will often not be apparent until the autopsy, unless the patient suffered from a heart condition which is known to cause sudden cardiac death
- The term “sudden death” is used until it is confirmed or deemed most likely that the cause was cardiac
- 50% of cardiac arrests occur in individuals with coronary artery disease which has not been discovered
- Etiology
- Coronary artery disease
- Valvular heart disease
- Myocarditis
- Hypertrophic cardiomyopathy
- Arrhythmogenic right ventricular cardiomyopathy
- Pathophysiology
- ~50% of SCD is caused by arrhythmias
- Most cases are due to ventricular arrhythmias following AMI
- ~50% of SCD is caused by acute heart failure
- ~50% of SCD is caused by arrhythmias
- Primary prevention with ICD
- Patients with heart failure and cardiomyopathy are at high risk for ventricular arrhythmias, meaning that primary prevention of SCD is important in these patients
- Patients who fulfil all the following criteria:
- Symptomatic HF (class II or III)
- LVEF < 35%
- Have tried 3 months of optimal medical therapy without improvement of above parameters
- High chance that they will survive more than 1 year with good functional status
- These patients should receive an ICD
- Primary prevention with CRT-D
- Patients who fulfil all the following criteria:
- Mildly symptomatic HF (class II)
- LVEF < 30%
- QRS > 130 ms
- Have LBBB
- Have tried 3 months of optimal medical therapy without improvement of above parameters
- High chance that they will survive more than 1 year with good functional status
- These patients should receive CRT-D
- Patients who fulfil all the following criteria:
- Secondary prevention with ICD
- Patients who fulfil all the following criteria:
- Have experienced cardiac arrest which was not due to reversible causes
- High chance that they will survive more than 1 year with good functional status
- These patients should receive an ICD
- Patients who fulfil all the following criteria:
- Cardiac arrest refers to a sudden, unexpected cessation of cardiac activity, causing haemodynamic collapse
11. Antiarrhythmic drugs
- Principles in antiarrhythmic therapy
- Most antiarrhythmic drugs have proarrhythmic effect and therefore increase mortality
- They can cause new arrhythmias or worsen current arrhythmias
- We treat fewer patients with arrhythmias
- Some arrhythmias cannot be treated by drugs
- Not all arrhythmias need to be treated at all
- We should look for underlying causes, like hyperthyroidism, ischaemic heart disease
- Non-pharmacological treatment is now more important
- For most antiarrhythmic drugs it’s important to follow up with Holter, exercise stress test, etc
- The only exception is amiodarone, which is not proarrhythmic and therefore can be given empirically
- Consideration of the risk-benefit ratio is important
- Side effects should be monitored
- Especially amiodarone has severe extracardiac side effects
- Most antiarrhythmic drugs have proarrhythmic effect and therefore increase mortality
- Vaughan Williams
- I/A
- (Quinidine)
- Procainamide
- Disopyramide
- I/B
- Lidocaine
- Mexiletine
- I/C
- Flecainide
- Propafenone
- II
- Metoprolol
- Bisoprolol
- Esmolol
- Nebivolol
- III
- Amiodarone
- Sotalol
- Dronedarone
- Less effective than amiodarone
- More hepatotoxic
- IV
- Verapamil
- Diltiazem
- I/A
- Other
- Magnesium sulphate
- Stabilizes membrane potential
- Used as adjunctive therapy in many arrhythmias
- Vernakalant
- Atrial-selective
- Magnesium sulphate
12. Pacemakers and implantable cardioverter defibrillators (ICD)
- See topic 25 in surgery 1
13. Epidemiology and risk factors of ischemic heart disease (IHD), primary prevention
- Epidemiology
- IHD is the leading cause of death in the world
- Males
- 2 – 5 % of males under 55
- 10 – 20 % of males over 65
- Females
- 1 % of females under 55
- 10 – 15 % of females over 65
- Annual mortality rate is 1 %
- Annual myocardial infarction rate is 1 – 2 %
- 25 million people may die from IHD in 2020
- Risk factors
- Classic risk factors
- Male gender
- Old age
- Dyslipidaemia
- High total cholesterol
- High LDL cholesterol
- Low HDL cholesterol
- Hypertension
- Smoking
- Diabetes mellitus
- Obesity
- Positive family history
- New risk factors
- Chronic kidney disease
- Bad diet
- Elevated CRP
- Hyperuricaemia
- Hyperhomocysteinaemia
- Microalbuminuria
- Classic risk factors
- Primary risk stratification
- Systematic cardiovascular risk assessment is recommended in everyone with known CV risk factors, or comorbidities which increase CV risk
- See risk factors above
- Systematic cardiovascular risk assessment is recommended for all adults > 40 years, even if they are healthy and have no known CV risk factors
- The SCORE system estimates the risk for fatal cardiovascular disease within 10 years, depending on the following factors:
- Gender
- Age
- Smoking
- Systolic blood pressure
- Total cholesterol
- There are two different SCORE charts, one for countries at low CV risk and one for countries at high CV risk
- Some of the countries at low CV risk
- Scandinavian countries
- UK
- Mediterranean countries
- Germany
- Some of the countries at high CV risk
- Hungary
- Russia
- Czechia
- Poland
- Croatia
- Some of the countries at low CV risk
- Some individual risk factors are so significant that they can decide the CV risk category for the patient regardless of SCORE risk
- For example, a patient with diabetes mellitus but a SCORE risk of 1% has high CV risk
- Low and moderate CV risk persons
- The following factors place the patient in the low or moderate CV risk category
- SCORE risk < 5%
- Management
- Should be offered lifestyle advice to maintain their low risk
- The following factors place the patient in the low or moderate CV risk category
- High CV risk persons
- The following factors place the patient in the high CV risk category
- SCORE risk 5 – 10 %
- Markedly elevated single risk factors
- Diabetes mellitus
- Moderate chronic kidney disease
- Management
- Should be offered intensive lifestyle advice
- May be candidates for drug treatment
- The following factors place the patient in the high CV risk category
- Very high CV risk persons
- The following factors place the patient in the very high CV risk category
- SCORE risk > 10 %
- Documented cardiovascular disease
- Previous AMI
- ACS
- Previous PCI
- Stroke or TIA
- Aortic aneurysm
- PAD
- Diabetes mellitus with target organ damage
- Severe chronic kidney disease (GFR < 30)
- Management
- Drug treatment is frequently required
- The following factors place the patient in the very high CV risk category
- Systematic cardiovascular risk assessment is recommended in everyone with known CV risk factors, or comorbidities which increase CV risk
- Treatment targets
- Smoking cessation
- Dietary changes
- Low in saturated fat
- More wholegrain products, vegetables, fruit, fish
- Physical activity
- 150 minutes a week of moderate physical activity or:
- 75 minutes a week of vigorous physical activity
- Body weight
- BMI 20 – 25
- Waist circumference < 94 cm in men, < 80 cm in women
- Blood pressure
- < 140/90 mmHg
- LDL cholesterol
- Low and moderate risk persons: < 3,0 mM
- High risk persons: < 2,6 mM
- Very high-risk persons < 1,8 mM
- HbA1c
- < 7 % (< 53 mmol/mol)
- Prevention measures
- Counselling
- In those who are not very high risk, counselling and lifestyle changes should always be tried for some time before drug therapy
- Statin therapy
- Antihypertensive therapy
- Counselling
14. Types of ischemic heart disease (IHD) (types of angina pectoris)
- Ischaemic heart disease
- An umbrella term for all diseases which are the result of ischaemia of myocardium
- Chronic coronary syndromes (CCS) (sometimes called stable ischaemic heart disease (SIHD)
- Angina pectoris (exertional angina)
- Dyspnoea
- CCS can manifest as only dyspnoea, especially in diabetic patients
- Acute coronary syndromes (ACS)
- Unstable angina
- NSTEMI
- STEMI
- Chronic coronary syndromes (CCS) (sometimes called stable ischaemic heart disease (SIHD)
- Due to coronary artery disease in the vast majority of cases
- Because of this coronary artery disease and ischaemic heart disease are often used interchangeably
- Even though ACS are technically ischaemic heart diseases, the term “ischaemic heart disease” most commonly refers to the chronic coronary syndromes
- An umbrella term for all diseases which are the result of ischaemia of myocardium
- Clinical classification of chest pain
- Typical angina (all 3 characteristics are present)
- Substernal pain with compressing characteristic
- Pain is provoked by exertion, stress, overeating
- Pain is relieved by rest or nitroglycerine
- Atypical angina
- Only 2 of the above characteristics are present
- Non-anginal chest pain
- Only 1 of the above characteristics are present
- Paradoxically, only 10 – 15 % of patients suspected for IHD present with typical angina
- Typical angina (all 3 characteristics are present)
15. The diagnostics of ischemic heart disease (IHD)
- Diagnostic workup of a patient in whom there is suspicion of IHD
- Step 1 – assess symptoms and perform clinical examination and anamnesis
- Typical angina makes the diagnosis almost certain
- Step 2 – consider comorbidities and patient’s general health
- Important for risk stratification, diagnostic options and treatment options
- Step 3
- Resting ECG
- Often normal if patient doesn’t currently have angina
- May reveal past infarcts
- Initial lab test
- CBC
- Glucose and HbA1c
- Lipid profile
- Renal function
- TSH
- Troponins
- To exclude ACS
- Ultra-sensitive troponin assays may detect slight elevation of troponins in CCS, which is associated with worse prognosis
- Echocardiography
- Abnormal ventricular function indicates IHD
- Can exclude other causes of chest pain, like HF, valve disease, cardiomyopathy
- Measurement of LVEF is important for risk stratification
- Chest x-ray
- If there is suspicion of pulmonary disease or HF
- Resting ECG
- Step 4 – assess pre-test probability and clinical likelihood of IHD
- The pre-test probability of the patient having IHD is determined based on the results of the above examinations
- Tables like this may help in assessing the pre-test probability
- If the pre-test probability is very low, no diagnostic testing is needed
- It can be assumed that the patient doesn’t have IHD
- If the pre-test probability is very high, no diagnostic testing is needed
- It can be assumed that the patient has IHD
- If the pre-test probability is anywhere in between, diagnostic testing is needed
- The pre-test probability of the patient having IHD is determined based on the results of the above examinations
- Step 5 – diagnostic testing which establishes the diagnosis of IHD
- If the pre-test probability is high, the patient should be referred to invasive coronary angiography
- During the angiography PCI can be carried out if necessary
- If the pre-test probability is intermediate, the patient should be referred to non-invasive imaging to test for ischaemia
- Stress testing (exercise or pharmacological stress)
- ECG, echo, SPECT, PET
- If the pre-test probability is low, the patient should be referred to coronary CT angiography
- If the pre-test probability is high, the patient should be referred to invasive coronary angiography
- Step 6 – patient’s risk for future cardiovascular events is determined
- This risk has major impacts on choice of therapy
- Those at high risk will have higher benefit of revascularization (PCI, CABG) therapy
- Risk is determined based on result from angiography, exercise ECG, echo, etc.
- Step 1 – assess symptoms and perform clinical examination and anamnesis
16. The drug treatment of ischemic heart disease (IHD)
- Drug treatment of ischaemic heart disease
- Drug therapy is the main treatment for all patients
- Aims
- To improve prognosis (prevent future myocardial infarction and death)
- To improve symptoms
- Drugs which improve prognosis (by preventing future CV events)
- Aspirin 75 – 100 mg daily
- In those patients who had AMI or underwent revascularization
- Clopidogrel if aspirin is not tolerated
- Statins
- In all patients with CCS
- If lipid goal is not achieved with max dose of statins -> add ezetimibe
- If lipid goal is not achieved with statin + ezetimibe -> add PCSK9 inhibitor (alirocumab)
- ACE inhibitors
- In patients with CCS who also have heart failure, hypertension or diabetes
- Beta blockers
- In patients with CCS who also have LV dysfunction or heart failure
- Aspirin 75 – 100 mg daily
- Drugs which improve symptoms
- Short-acting nitrates
- For immediate relief of angina
- Beta-blockers and/or CCBs
- First line to control symptoms
- Short-acting nitrates
17. The revascularisation treatment (PCI, CABG) of ischemic heart disease (IHD)
- Revascularization (PCI, CABG)
- Revascularization provides no or modest benefit in most patients with CCS
- Because the risk outweighs the benefit in these cases, revascularization is reserved for certain cases
- Indicated in
- Patients with CAD in whom symptoms persist despite optimal medical therapy
- Patients with CAD in whom revascularization has been proven to improve the prognosis
- Left main coronary artery stenosis > 50%
- Proximal LAD stenosis > 50%
- Multi-vessel disease with impaired LV function
- Patients with STEMI
- Patients with NSTEMI at high risk
- The choice between PCI and CABG for CCS is not always easy
- For ACS the choice is virtually always PCI
- The so-called SYNTAX score scores the complexity of coronary artery disease and is used to guide the choice between PCI and CABG
- A higher SYNTAX score indicates a more complex coronary artery disease
- Conditions which favour PCI over CABG
- Severe co-morbidities
- Advanced age/frail patient/reduced life expectancy
- Multi-vessel disease with low SYNTAX score
- Coronary anatomy which will likely result in incomplete revascularization with CABG
- Conditions which favour CABG over PCI
- Patients with diabetes
- Reduced LVEF (< 35%)
- Contraindications to DAPT
- Multi-vessel disease with intermediate or high SYNTAX score
- Coronary anatomy which will likely result in incomplete revascularization with PCI
- Revascularization provides no or modest benefit in most patients with CCS
- Percutaneous coronary intervention (PCI)
- Procedure
- The coronaries are catheterized like during coronary angiography
- A balloon catheter is inflated at the site of the coronary occlusion
- The inflated balloon will dilate the occlusion
- In most cases a stent will be inserted to keep the occlusion open afterward
- The stent can be bare-metal or drug-eluting
- Drug-eluting stents are recommended over bare metal stents
- Drug-eluting stents elute drugs like everolimus or sirolimus a few months after it is placed
- This prevents intimal hyperplasia, which reduces the risk of in-stent stenosis
- After PCI
- Echocardiography
- In all patients
- To assess ventricular function, detect post-MI complications
- Antithrombotic therapy
- See “secondary prevention” under topic 22
- DAPT for 6 months, followed by life-long aspirin
- Echocardiography
- Procedure
- Fibrinolytic therapy
- Indicated for STEMI and ACS with OMI if the patient cannot be brought to a PCI lab within 120 minutes of diagnosis
- Fibrinolytic therapy should be initiated within 10 minutes of diagnosis
- Patient must receive UFH or enoxaparin before hand
- tPAs like tenecteplase, alteplase or reteplase are used
- Patient should be transferred to a PCI-capable hospital immediately after fibrinolysis
- Contraindications
- Recent stroke or TIA
- CNS damage
- CNS tumour
- Recent major trauma or surgery
- Recent GI bleeding
- Pregnancy
- Patient on oral anticoagulant therapy
- Indicated for STEMI and ACS with OMI if the patient cannot be brought to a PCI lab within 120 minutes of diagnosis
- CABG
- See surgery 1 topic 20
18. Types and diagnostics of acute coronary syndromes (ACS)
- Acute coronary syndrome (ACS)
- An umbrella term for three conditions
- Unstable angina, NSTEMI, STEMI
- All three have similar clinical features
- They cannot be differentiated based on clinical features and must be differentiated based on troponin level and ECG
- A different classification has been proposed but is not in widespread use:
- Acute coronary syndrome with ongoing myocardial ischaemia (ACS with OMI)
- Myocardial infarctions which do not resolve before the first medical contact, and with at least one of the following findings of ongoing myocardial ischaemia:
- Significant ST elevations or depressions
- New bundle branch block
- Cardiogenic shock
- Malignant arrhythmias
- Acute heart failure
- New wall motion abnormality visible on cardiac imaging
- Acute coronary syndrome without ongoing myocardial ischaemia (ACS without OMI)
- Unstable angina or small infarcts which resolve before the first medical contact
- Acute coronary syndrome with ongoing myocardial ischaemia (ACS with OMI)
- Clinical features
- Angina at rest
- Often described as squeezing, tightness, pressure, etc.
- Sometimes described more as a discomfort than a pain
- The pain is diffuse and difficult to localize to one specific spot
- May radiate anywhere
- To upper extremities
- To shoulders
- To lower jaw
- An old saying (which is true) is that “pain above the nose or below the navel is rarely cardiac in origin”
- Dyspnoea
- Atypical symptoms
- Atypical chest pain
- Pleuritic or sharp pain
- Pain in the mid or lower abdominal region
- Dyspnoea
- Nausea
- Vomiting
- Epigastric pain
- Palpitation
- Atypical chest pain
- 1/3 of patients with myocardial infarction present without chest pain but with atypical symptoms alone
- This is more common in elderly, diabetics, and women
- Angina at rest
- Procedure at first medical contact (FMC)
- Diagnosis
- ECG
- Blood sample
- Especially troponins
- Evaluation of ECG and diagnosis should take less than 10 minutes from FMC
- Initial therapy
- The initial therapy of ACS is often abbreviated MONA
- IV morphine
- Only if severe pain, as morphine worsens the outcome
- Sublingual nitroglycerine
- Oxygen
- If SaO2 < 90%
- Aspirin
- 150 – 300 mg oral loading dose
- Beta blocker
- Contraindicated in hypotension, heart failure, cardiogenic shock
- If the final diagnosis is STEMI -> topic 19
- If the final diagnosis is NSTEMI -> topic 20
- If the final diagnosis is unstable angina -> topic 20
- Diagnosis
- Unstable angina
- Non-ST-segment elevation myocardial infarction (NSTEMI)
- Acute myocardial ischaemia which causes subendocardial infarction, which is severe enough to elevate troponin and cause abnormal ECG but not severe enough to cause ST elevation
- It is due to a partial occlusion of a coronary artery
- But more severe than in unstable angina
- Diagnosis is based on the following:
- Clinical features of ACS
- Normal ECG or non-specific findings on ECG
- ST depression
- T inversion
- But no ST elevations
- Rise and/or fall in troponins
- NSTEMI and unstable angina are frequently indistinguishable at initial evaluation, because troponin elevation may not be detectable that early
- For this reason, ECG and blood sampling should be repeated regularly until no suspicion for NSTEMI remains
- ST-segment elevation myocardial infarction (STEMI)
- Acute myocardial ischaemia which causes transmural infarction, which is severe enough to elevate troponin and cause significant ST elevation and/or new bundle branch block
- It is due to a total occlusion of a coronary artery
- Diagnosis is based on the following:
- Clinical features of ACS
- Specific ECG findings. One of the following:
- Significant ST elevations in two contiguous leads
- New left or right bundle branch block
- Rise and/or fall in troponins
- An umbrella term for three conditions
- 5 Types of myocardial infarction
- Myocardial infarction type 1
- The “classic” type, which is due to atherosclerotic plaque rupture or erosion with a resulting thrombus
- Myocardial infarction type 2
- A condition other than coronary artery disease causes an acute imbalance between myocardial oxygen supply and oxygen demand
- Causes of acute decreased oxygen supply
- Hypoxaemia
- Severe anaemia
- Hypotension
- Coronary artery spasm
- Coronary artery embolism
- Causes of acute increased oxygen demand
- Tachyarrhythmias
- Hypertension
- Myocardial infarction type 3
- Sudden cardiac death due to myocardial infarction
- Death occurs before biomarkers could be sampled from blood
- Myocardial infarction type 4
- Myocardial infarction during PCI, or due to a stent thrombosis after PCI
- Myocardial infarction type 5
- Myocardial infarction during CABG
- Myocardial infarction type 1
- Morphological types of myocardial necrosis according to MRi
- Ischaemic injury (infarction)
- Transmural – corresponds to STEMI
- Subendocardial or focal subendocardial – corresponds to NSTEMI
- Non-ischaemic injury
- Due to non-ischaemic causes, like myocarditis, amyloidosis, sarcoidosis, etc.
- Subepicardial
- Mid-wall
- Insertion points
- Injuries at the insertion point where the right ventricle connects to the left ventricle
- Ischaemic injury (infarction)
- Myocardial infarction with non-obstructive coronary arteries (MINOCA)
- A myocardial infarction, but no coronary arteries with more than 50% obstruction can be found on angiography, and no other clear cause of the infarction can initially be found
- Accounts for 1 – 14% of myocardial infarctions
- Not much is known about causes and therapy
- Potential underlying causes
- Coronary spasm
- Coronary microvascular disorders
- Slow coronary flow
- Microvascular spasm
- Plaque disruption
- Spontaneous thrombus/embolus
- Myocarditis
- Takotsubo cardiomyopathy
- Etc.
19. The treatment of acute coronary syndromes with ST segment elevation (STEMI)
- If ST elevations and typical symptoms are found at FMC, the diagnosis is STEMI
- We don’t wait for troponins if ST elevations and typical symptoms are present
- If the diagnosis at FMC is STEMI (or ACS with OMI but without ST elevation), and:
- The time it would take to bring the patient to an angiography lab is < 120 minutes
- -> the patient should be brought there and primary PCI should be performed
- The time it would take to bring the patient to an angio lab is > 120 minutes
- -> fibrinolytic therapy should be initiated immediately -> patient should be brought to angio lab to evaluate whether PCI is necessary
- The time it would take to bring the patient to an angiography lab is < 120 minutes
- Primary PCI refers to emergency PCI performed on the infarct-related artery (IRA) on patients with myocardial infarction
- Antithrombotic therapy
- Aspirin should already have been given at FMC
- P2Y12 inhibitor (like prasugrel or clopidogrel) and unfractionated heparin should be initiated before PCI
20. The treatment of acute coronary syndromes without persistent ST segment elevation (NSTEMI)
- NSTEMI and unstable angina are frequently indistinguishable at initial evaluation, because troponin elevation may not be detectable that early
- For this reason, the initial treatment of these conditions is the same
- Fibrinolysis is never performed for NSTEMI
- Antithrombotic therapy
- Aspirin should already have been given at FMC
- Like for STEMI, P2Y12 inhibitor and unfractionated heparin should be started
- Early risk stratification of the patient should be performed
- This means risk score systems are used to identify the patient’s risk for later cardiac events, like sudden cardiac death
- The higher the risk, the sooner the patient must be taken to coronary angiography
- The results of the angiography will determine whether a PCI will be performed at the same procedure as well
- Multiple risk score systems exist, like TIMI and GRACE
- See also topic 22
- If the result of the early risk stratification determines that the patient is extremely high risk the patient should be sent immediately (< 2 hours) to coronary angiography at a PCI lab
- Factors which indicate extremely high risk
- Cardiogenic shock
- Acute heart failure
- Haemodynamic instability
- Ventricular arrhythmia
- Factors which indicate extremely high risk
- If the result of the early risk stratification determines that the patient is high risk the patient should be sent to coronary angiography within 24 – 48 hours
- If the result of the early risk stratification determines that the patient is intermediate risk the patient should be sent to coronary angiography within 72 hours
21. The most important complications of acute myocardial infarction (AMI) and their treatment
- Arrhythmias
- Usually occur within 24 hours of infarction
- May be due to ischaemia of the conduction system or due to autonomic imbalance (often sympathetic overactivation)
- Most commonly bradyarrhythmias or conduction disturbances
- Many arrhythmias are transient, resolving after revascularization of the infarct
- Treatment
- Atropine
- Bradyarrhythmias
- Beta blocker
- Atrial fibrillation (if rhythm control is needed)
- Ventricular arrhythmias
- Temporary pacemaker
- Mobitz type II 2nd degree AV block
- 3rd degree AV block
- Asystole
- Atropine
- If the arrhythmias don’t resolve a permanent pacemaker may be necessary
- Early infarct-associated pericarditis
- Mechanical complications
- More common in STEMI than NSTEMI
- Usually occur 3 – 14 days after infarction
- Mechanical complications often lead to cardiogenic shock, so diagnosis and treatment is urgent
- Rupture of ventricular free wall
- Complete rupture often causes death almost immediately
- Incomplete rupture can cause hemopericardium with tamponade
- Rupture of interventricular septum
- Papillary muscle rupture
- Rupture of the papillary muscles causes acute mitral regurgitation
- Diagnosis
- Echocardiography
- Treatment
- Surgical repair
- Late complications
- Ventricular aneurysm
- Postmyocardial infarction syndrome (Dressler syndrome)
- Autoimmune pericarditis
- Ischaemic cardiomyopathy -> heart failure
22. Risk stratification after acute myocardial infarction (AMI), secondary prevention
- Risk stratification after AMI
- Risk stratification means evaluating the patient’s risk for adverse outcomes, like death
- Patients with ACS should undergo both early and late risk stratification
- Early risk stratification
- Should be performed as early as possible after diagnosis
- Important to determine treatment options and to evaluate prognosis
- TIMI or GRACE risk score are often used
- Late risk stratification
- Should be performed at the time of discharge or a few weeks after
- Long-term management and prognosis depend on this
- Includes measurement of LVEF, sometimes stress testing
- Measurement of LVEF is indicated in all patients with AMI before discharge, and 6 – 12 weeks after the AMI
- LVEF < 35% indicates higher risk for mortality
- Stress testing can detect residual ischaemia, which signals higher risk for mortality
- Secondary prevention
- Secondary prevention means the therapies which aim to prevent further cardiovascular events in the future
- Antithrombotic therapy after PCI after AMI
- This reduces the risk of stent thrombosis
- DAPT with low-dose aspirin and P2Y12 inhibitor
- A PPI should be added in people with high risk for GI bleeding
- For patients with low bleeding risk DAPT should last 6 – 12 months
- After this the P2Y12 inhibitor is discontinued, but the patient remains on aspirin indefinitely
- Lipid-lowering therapy after AMI
- Blood lipid levels should be obtained asap in all STEMI patients
- High-dose statin therapy should be initiated as early as possible and maintained long-term
- It is recommended to reach one of the following LDL targets:
- LDL < 1,8 mM
- A reduction in LDL of at least 50% if the LDL was already between 1,8 and 3,5 mM
- If these targets are unattainable with only statins, other agents, like ezetimibe, should be added
- Antihypertensive treatment
- Goal is < 140/90 mmHg
- In patients who also have LVEF < 40%
- ACEi, beta blockers, MRAs
- For secondary prevention of sudden cardiac death, see topic 10
- Cardiac rehabilitation
- See topic 44
23. Risk factors, pathogenesis, epidemiology, and types of hypertension.
- Definition of hypertension (HTN)
- The relationship between BP and cardiovascular and renal events is continuous, which makes the distinction between “normal” blood pressure and “high” blood pressure somewhat arbitrary
- In practice, the threshold for “high” blood pressure is defined as the level of BP where the benefits of treatment outweigh the risks, as documented by clinical trials
- BP measured in the office
- SBP > 140 mmHg and/or
- DBP > 90 mmHg
- Average BP measured by ambulatory blood pressure monitoring
- SBP > 130 mmHg and/or
- DBP > 80 mmHg
- Average BP measured during the daytime by ambulatory blood pressure monitoring
- SBP > 135 mmHg and/or
- DBP > 85 mmHg
- Average BP measured during the night-time by ambulatory blood pressure monitoring
- SBP > 120 mmHg and/or
- DBP > 70 mmHg
- Average BP measured by the patient during a 3 – 7-day period at home
- SBP > 135 mmHg and/or
- DBP >85 mmHg
- The relationship between BP and cardiovascular and renal events is continuous, which makes the distinction between “normal” blood pressure and “high” blood pressure somewhat arbitrary
- Risk factors for primary hypertension
- Old age
- Black race
- Positive family history
- Obesity
- Diabetes
- Smoking
- Alcohol abuse
- Diets high in sodium
- Physical inactivity
- Pathogenesis of primary hypertension
- The pathogenesis of primary hypertension is largely unknown
- Epidemiology of hypertension
- It is present in 15 – 30% of adults
- It is present in 30 – 40% of elderly
- In developed countries, only 1 in 4 to 1 in 8 patients with hypertension receive efficient blood pressure control
- Grades of hypertension (in SBP/DBP)
|
Grade |
Systolic (mmHg) | Diastolic (mmHg) | |
|
Optimal |
< 120 | And | < 80 |
| Normal | 120 – 129 | And/or |
80 – 84 |
|
High normal |
130 – 139 | And/or | 85 – 89 |
| Grade 1 hypertension | 140 – 159 | And/or |
90 – 99 |
|
Grade 2 hypertension |
160 – 179 | And/or | 100 – 109 |
| Grade 3 hypertension | > 180 | And/or |
> 110 |
| Isolated systolic hypertension | > 140 | And |
< 90 |
- Special types of hypertensions
- Primary (essential) hypertension
- Hypertension with no specific cause
- Accounts for 90% of hypertensive adults
- Accounts for 20% of hypertensive children (< 12 years)
- Secondary hypertension
- Hypertension with a specific cause
- Accounts for 10% of hypertensive adults
- Accounts for 80% of hypertensive children (< 12 years)
- Causes
- Primary hyperaldosteronism
- Most common cause of secondary HTN
- Sleep apnoea syndrome
- Parenchymal or vascular kidney disease
- Pheochromocytoma
- Cushing syndrome
- Illegal drug abuse
- Etc.
- Primary hyperaldosteronism
- White coat hypertension
- When the patient measures > 140/90 mmHg at the office but is normotensive on ABPM or during home measurements
- No treatment required, just follow-up
- Masked hypertension
- Basically the opposite of white coat hypertension
- When the patient measures < 140/90 mmHg at the office but is hypertensive on ABPM or during home measurements
- Treated as normal hypertension
- Hypertensive urgency
- = An acute increase in BP to > 180 mmHg SBP or > 120 mmHg DBP, but without signs of hypertension-mediated organ damage
- Is often due to non-adherence to antihypertensive drugs in patients who are hypertensive
- Does not need hospital admission
- Can be treated as any other HTN, but requires urgent outpatient monitoring to ensure the BP comes under control
- Hypertensive emergency
- = An acute increase in BP to > 180 mmHg SBP or > 120 mmHg DBP, and with signs of hypertension-mediated organ damage
- Hypertensive retinopathy
- Blurry vision
- Retinal haemorrhage
- Papilledema
- Myocardial infarction
- Heart failure exacerbation/pulmonary oedema
- Hypertensive encephalopathy
- Headache
- Vomiting
- Stroke
- Acute renal failure
- Hypertensive retinopathy
- Needs hospital admission
- BP must be normalized slowly to allow autoregulated organs to reset their autoregulatory threshold
- Except if there is pre-eclampsia, eclampsia, aortic dissection, pheochromocytoma, pulmonary oedema, myocardial infarction or hypertensive encephalopathy, in which case the BP must be reduced immediately
- = An acute increase in BP to > 180 mmHg SBP or > 120 mmHg DBP, and with signs of hypertension-mediated organ damage
- Primary (essential) hypertension
24. The treatment of hypertension
- Blood pressure target values
- < 140/90 mmHg in most cases
- < 140/85 mmHg in diabetics
- Nonpharmacological therapy
- Should always be offered to the patient
- Smoking cessation
- Weight loss
- Decrease salt intake (< 5 g/day)
- Restrict alcohol
- Improve diet
- Exercise
- Pharmacological therapy
- Indications
- All grade 2 and 3 hypertensive patients
- Grade 1 hypertensive patients
- in which nonpharmacological therapy didn’t reduce BP satisfactorily
- who are at high risk for hypertensive organ damage
- Monotherapy is often insufficient reach BP target values
- Monotherapy is only used in very old hypertensive patients, or grade 1 hypertensive patients
- In all other patients, combination therapy of different drug classes is used
- Single pill combinations of two or more antihypertensive drugs are often used
- Drug choice is based on contraindications of the drugs, and if the patient has any comorbidities which are indications for the drug
- Diuretics
- MRB, thiazides
- Beneficial in
- Heart failure
- Elderly
- Isolated hypertension
- Beta blockers
- Beneficial in
- Coronary artery disease
- Tachyarrhythmia
- Post-AMI, heart failure
- These patients should be on beta blockers even if they don’t have HTN
- Contraindicated in
- Asthma
- COPD
- Bradyarrhythmia
- Beneficial in
- ACEi/ARB
- Beneficial in
- Diabetic nephropathy
- Post-AMI, heart failure
- These patients should be on ACEi even if they don’t have HTN
- Contraindicated in
- Pregnancy
- Beneficial in
- Calcium channel blockers
- Beneficial in
- Coronary artery disease
- Vasospastic disease
- Pulmonary arterial hypertension
- Elderly
- Contraindicated in
- Bradyarrhythmia
- Beneficial in
- Alpha blockers
- Generally not a first choice
- Beneficial in BPH
- Indications
25. Epidemiology, risk factors and pathomechanism of heart failure
- Heart failure = a clinical syndrome where the ventricles can’t fill with blood or eject blood
- Mortality without medical therapy – 50%
- Mortality with optimal medical therapy – 7%
- Risk factors
- Smoking, COPD
- Diabetes mellitus
- Obesity
- Arrhythmias
- Etiology
- Intrinsic myocardial disease
- Myocardial infarction
- Cardiomyopathy
- Myocarditis
- Toxic agents
- Alcohol
- Cocaine
- Anthracyclines
- Cyclophosphamide
- Radiation
- Excess cardiac workload
- Pressure overload
- Hypertension
- Aortic or pulmonary stenosis
- Hypertrophic cardiomyopathy
- Volume overload
- Aortic insufficiency
- Mitral insufficiency
- Tricuspid insufficiency
- Congenital left-to-right shunts
- Pressure overload
- Increased body demand of CO (“high output heart failure”)
- Thyrotoxicosis
- Anaemia
- Pregnancy
- AV fistula
- Intrinsic myocardial disease
- Pathomechanism
- According to the Frank-Starling mechanism, dilation of the ventricles increases the contractility, but only up to a point
- Beyond this point, further dilation reduces the contractility
- Activation of neurohumoral systems
- Increased sympathetic activity
- Decreases contractility
- Causes apoptosis of cardiac myocytes
- Precipitates arrhythmias
- Increases myocardial fibrosis
- Causes peripheral vasoconstriction
- Activation of RAAS
- Increases myocardial fibrosis
- Increases water and salt retention
- Release of natriuretic peptides (BNP, ANP)
- Increased sympathetic activity
- Activation of RAAS and the SNS stimulate myocardial remodelling, which involves:
- Myocardial hypertrophy
- Chamber dilation
- Abnormal chamber geometry
- Increased myocardial fibrosis
- Myocardial remodelling eventually causes ventricular dysfunction
- According to the Frank-Starling mechanism, dilation of the ventricles increases the contractility, but only up to a point
26. The clinical syndromes of heart failure
- New York Heart Association (NYHA) classification of heart failure
- NYHA class I
- Symptoms of heart failure only in excessive exercise, or no symptoms of heart failure at all
- NYHA class II
- Symptoms of heart failure during normal daily activity like climbing stairs, making food, etc.
- NYHA class III
- Symptoms of heart failure during easy daily activity like dressing, walking on flat surface
- NYHA class IV
- Symptoms present during rest
- NYHA class I
- Types of heart failure
- Heart failure with preserved ejection fraction (HFpEF)
- Previously known as diastolic heart failure
- Ejection fraction > 50%
- Heart failure with midrange ejection fraction (HFmrEF)
- Ejection fraction 40 – 50%
- Heart failure with reduced ejection fraction (HFrEF)
- Previously known as systolic heart failure
- Ejection fraction < 40%
- Heart failure with preserved ejection fraction (HFpEF)
- Diagnosis of heart failure
- Heart failure is a clinical diagnosis
- Labs and imaging are used to evaluate the severity and etiology, but evidence of cardiac dysfunction on echo is essential for the diagnosis
- ECG
- 90% of patients with HF will have some type of ECG abnormality
- Left ventricular hypertrophy, arrhythmias, BBBs, etc.
- A normal ECG means HF is unlikely
- 90% of patients with HF will have some type of ECG abnormality
- Chest x-ray
- Unreliable
- Can differentiate whether dyspnoea is cardiac or pulmonary in origin
- Signs
- Kerley B lines
- Cardiomegaly
- Cardiothoracic ratio > 0,5
- Apicobasal calliper discrepancy
- Echocardiography
- Transthoracic (TTE) or transoesophageal (TEE)
- Gold standard for assessing cardiac function and morphology
- Gives the ejection fraction
- Almost always tells you the etiology
- Valvular disease
- Wall motion disorders
- Can indicate prior or acute myocardial infarction
- Myocardial thickness
- Interventricular septum normally < 11 mm
- Diastolic function
- Diastolic filling
- Ventricle dilatation
- Chamber sizes
- Labs
- NTpro-BNP or BNP
- CBC
- May show anaemia
- Liver function
- Electrolytes
- More severe hyponatraemia -> worse prognosis
- Degree of hyponatraemia correlates with severity
- CRP
- Renal function
- TSH
- Glucose and HbA1c
- To screen for diabetes
- Lipids and cholesterol
- To screen for dyslipidaemia
- Heart failure is a clinical diagnosis
- Clinical features of heart failure
- General features
- Cardiac cachexia
- Fatigue
- Pulsus alternans
- Tachycardia
- Features of left-sided heart failure
- Pulmonary symptoms dominate
- Dyspnoea
- Orthopnoea
- Cardiac asthma
- Paroxysmal nocturnal dyspnoea
- Features of right-sided heart failure
- Congestive symptoms dominate
- Peripheral pitting oedema
- Jugular vein distension
- Hepatosplenomegaly
- Jaundice
- Ascites
- Loss of appetite
- General features
- Arrhythmias in HF
- Arrhythmias can worsen HF and increase mortality
- Tachyarrhythmias like Afib deplete cardiac myocytes of energy and stimulate myocardial remodelling
- Ventricular arrhythmias can cause sudden cardiac death
- Conduction abnormalities like BBB, AV block causes desynchronization of the chambers of the heart, which reduces CO and can cause volume and pressure overload
27. The drug treatment of chronic heart failure
- Treatment of underlying disease
- Myocardial ischaemia (coronary artery disease)
- Hypertension
- DM2
- Hyperthyroidism
- Drugs which improve prognosis:
- β-blockers
- Carvedilol
- Bisoprolol
- Metoprolol
- ACEI
- ACE inhibitors are preferred over other RAAS-inhibiting drugs because ACE also breaks down bradykinin
- Therefore, ACEI drugs increase the level of bradykinin, which is vasodilatory and therefore beneficial in HF
- ARBs (angiotensin II receptor blockers)
- Only used when ACEIs are not tolerated
- They’re otherwise inferior to ACEIs
- Mineralocorticoid receptor antagonists (MRAs)
- Spironolactone
- Eplerenone
- Angiotensin receptor-Neprilysin Inhibitors (ARNIs)
- Valsartan + Sacubitril (Trade name Entresto)
- Neprilysin is an enzyme which degrades bradykinin, ANP and BNP
- Sacubitril inhibits neprilysin, thereby increasing the level of these hormones
- β-blockers
- Drugs which improve symptoms
- Diuretics
- Furosemide
- Digoxin
- Diuretics
- Standard treatment of HFrEF
- Standard
- β-blocker
- Should only be initiated when the patient is stable and compensated
- ACEI
- β-blocker
- If above is not enough:
- MRA
- If above is not enough:
- If sinus rhythm and normal QRS: ivabradine
- If sinus rhythm and prolonged QRS: Cardiac resynchronization therapy (CRT)
- If not sinus rhythm: ARNI
- Standard
- Treatment of HFpEF and HFmrEF
- Treated as HFrEF
- Not as much research is done on these forms of HF, therefore we don’t quite know the best therapy yet
- Future treatments
- SGLT2 inhibitors (gliflozins) shows promise in HF, with or without DM2
28. The non-pharmacological treatment of heart failure
- Avoid certain medications
- NSAIDs
- Antiarrhythmic drugs
- Except amiodarone
- Calcium channel blockers
- Except amlodipine
- Tricyclic antidepressants
- Steroids
- General advices
- Regular self-weighing
- Used to monitor fluid balance
- In case of obesity: weight reduction
- Avoid extreme temperatures
- Restrict salt intake (< 3 g/day)
- Restrict water intake (1,5 L/day)
- Restrict alcohol
- Aerobic exercise
- Markedly increases quality of life in HF
- Regular self-weighing
- ICD – implantable cardioverter-defibrillator
- For primary prevention of sudden cardiac death in people with HF
- See topic 10 and surgery 1 topic 25
- Surgical treatment
- See surgery 1 topic 24
Acute heart failure
- Acute (decompensated) heart failure = Rapid onset of clinical signs and symptoms of heart failure
- Can either be the first occurrence of a new (de novo) heart failure or, more commonly, a decompensation of a chronic heart failure
- It is life-threatening and requires urgent treatment
- Etiology
- (These are factors which trigger decompensation or cause rapid-onset new heart failure)
- Acute coronary syndrome
- Tachyarrhythmias
- Atrial fibrillation
- Ventricular tachycardia
- Bradyarrhythmias
- Hypertensive emergency
- Infection
- Non-adherence to salt/fluid intake restrictions
- Non-adherence to medications
- Alcohol
- Pulmonary embolism
- Stress
- Exacerbation of COPD
- Thyroid dysfunction
- Pregnancy
- Cerebrovascular disease
- Clinical features
- Symptoms of congestion
- Orthopnoea
- Pulmonary congestion
- Peripheral oedema
- Etc.
- Symptoms of hypoperfusion
- Cold extremities
- Oliguria
- Mental confusion
- Symptoms of congestion
- Haemodynamic profiles
- Patients who have symptoms of congestion are “wet”, while those that don’t are “dry”
- 95% of acute heart failure patients are wet upon presentation
- Patients who have symptoms of hypoperfusion are “cold”, while those that don’t are “warm”
- Those patients who are warm and dry have the best prognosis, while those who are cold and wet have the worst prognosis
- The haemodynamic profile determines the treatment
- Patients who have symptoms of congestion are “wet”, while those that don’t are “dry”
29. The treatment of acute heart failure
- Examine for cardiogenic shock
- If yes, apply circulatory support
- Examine for respiratory failure
- If yes, apply ventilatory support
- Identify etiology and treat the underlying cause
- ACS -> PCI
- Hypertensive emergency -> antihypertensives
- Arrhythmia -> anti-arrhythmic treatment
- Acute mechanical cause (myocardial rupture, acute valvular disease) -> surgery
- Pulmonary embolism -> thrombolysis
- Etc.
- Diagnostic workup to confirm AHF
- Natriuretic peptides (NT-proBNP)
- Chest X-ray
- ECG
- Troponins
- Liver function, kidney function
- Electrolytes
- CBC
- Echocardiography
- If hypoxaemic (SpO2 < 90%) -> give O2
- Correct peripheral perfusion in “cold” patients
- Inotropic agents or vasopressors
- Dobutamine
- Milrinone
- Levosimendan
- Mechanical support if drugs are not sufficient
- Inotropic agents or vasopressors
- Correct congestive symptoms in “wet” patients
- Diuretics
- Loop diuretics
- Vasodilators
- Nitroglycerine
- Sodium nitroprusside
- Diuretics
- After stabilization, continue standard therapy for chronic heart failure
- For details on mechanical circulatory support like IABP, ECMO, see surgery 1 topic 24
30. Classification of cardiomyopathies
- Definition of cardiomyopathy
- According to ESC, cardiomyopathies are defined by structural and functional abnormalities of the ventricular myocardium that are unexplained by flow-limiting coronary artery disease or abnormal loading conditions
- This definition does not include diseases of the myocardium secondary to coronary artery disease or hypertension
- However, terms like “ischaemic cardiomyopathy” and “hypertensive cardiomyopathy” are used clinically, despite not being true cardiomyopathies according to the ESC definition
- Main cardiomyopathies
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Restrictive cardiomyopathy
- Arrhythmogenic right ventricular cardiomyopathy
- Other cardiomyopathies
- Tachycardia-induced cardiomyopathy
- Takotsubo cardiomyopathy
- Ischaemic cardiomyopathy
- Hypertensive cardiomyopathy
- Peripartum cardiomyopathy
31. Dilated cardiomyopathy (DCM)
- Dilated cardiomyopathy is the most common cardiomyopathy
- Etiology
- Idiopathic/genetic (50% of cases)
- 50% of those with idiopathic DCM have incidence of DCM in the family
- Myocarditis
- Often Coxsackie B
- Infiltrative disease
- Sarcoidosis
- Amyloidosis
- Alcohol/cocaine abuse
- Cardiotoxic drugs
- Wet beriberi
- Idiopathic/genetic (50% of cases)
- Pathophysiology
- Progressive eccentric hypertrophy causes dilation of the left ventricle, which decreases its contractility, eventually causing HF
- Ventricular dilation might cause functional mitral regurgitation, which worsens the heart failure
- Clinical features
- Symptoms of heart failure
- Diagnosis
- Echocardiography
- Shows dilated left ventricle and decreased LVEF
- Chest X-ray
- Cardiomegaly with “ballooning” left ventricle
- Echocardiography
- Treatment
- Treat underlying cause, if any
- Treat heart failure
- Primary prevention of SCD by ICD implantation
- Heart transplant
- DCM due to non-reversible causes are one of the most frequent causes of heart transplant
32. Hypertrophic and restrictive cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy
- Hypertrophic cardiomyopathy (HCM)
- Second most common cardiomyopathy
- HCM is a major cause of SCD in young patients
- Types
- Hypertrophic obstructive cardiomyopathy (HOCM) – 70% of cases
- Non-obstructive type – 30% of cases
- Often called just HCM, to distinguish it from HOCM
- Etiology
- Mutations in genes for sarcomeric proteins (60% of cases)
- The most frequent mutations are in the cardiac myosin binding protein-C gene or cardiac β-myosin heavy chain gene
- 50% of cases are familial
- Other known causes (10% of cases)
- Inborn errors of metabolism
- Neuromuscular diseases
- Mitochondrial diseases
- Etc.
- Idiopathic/unknown cause (30% of cases)
- Mutations in genes for sarcomeric proteins (60% of cases)
- Pathophysiology
- The myocardium is hypertrophic, remodelled and replaced by extracellular matrix and fibrosis
- Left ventricular outflow tract obstruction (LVOTO)
- Only in HOCM, hence the name
- The intraventricular septum hypertrophies more than the free LV wall
- The abnormally thick IV septum causes the fluid mechanics of the blood which is ejected during systole to be abnormal
- This causes the anterior leaflet of the mitral valve to be drawn against the septum and obstruct the left ventricular outflow tract
- Good figure on Amboss explaining it here
- This phenomenon occurs more frequently during exercise and stress
- Diastolic and systolic dysfunction
- In both obstructive and non-obstructive types
- The left ventricular hypertrophy and remodelling decreases the compliance of the myocardium and (paradoxically) reduces the contractility, too
- Arrhythmogenicity
- The changes to the myocardium increase the risk for arrhythmias like ventricular tachycardia and atrial fibrillation
- Clinical features
- Most have no or minor symptoms at diagnosis
- Dyspnoea
- Chest pain
- Syncope
- Palpitations
- Diagnosis
- Screening of first-degree relatives of affected patients
- Since many are asymptomatic many get diagnosed during family screening
- Physical examination
- Crescendo-decrescendo systolic ejection murmur
- S4 gallop
- Echocardiography
- Best initial and confirmatory test
- LV wall thickness > 15 mm
- In HOCM:
- Exercise beforehand may be necessary to provoke these findings
- Asymmetrically thickened IV septum
- Movement of the mitral valve towards the IV septum during systole
- Increased LVOT pressure gradient
- ECG
- Abnormal ECG signs may be the first sign of HCM
- Signs of left ventricular hypertrophy
- Screening of first-degree relatives of affected patients
- Complications
- Atrial fibrillation
- Due to arrhythmias or LVOTO
- Syncope
- Sudden cardiac death
- Due to systolic and/or diastolic ventricular dysfunction
- Heart failure
- Treatment
- Intense exercise is forbidden in all patients with HCM
- Pharmacological therapy
- Only for symptomatic patients
- Beta blockers (bisoprolol)
- Second line
- Verapamil, diltiazem
- Disopyramide
- Invasive treatment
- For symptomatic patients in which pharmacological therapy isn’t enough
- Ablation of hypertrophic myocardium with alcohol
- Surgical reduction of myocardium (myectomy)
- Management of co-existing comorbidities
- AF, HF, etc.
- Screening of 1st-degree relatives
- Prevention of SCD
- No intense exercise
- Secondary prevention with ICD
- See topic 10
- Primary prevention with ICD
- In those at high risk for SCD
- Restrictive cardiomyopathy (RCM)
- Definition
- Non-dilated ventricles with normal wall thickness
- Rigid ventricular walls resulting in severe diastolic dysfunction and restricted ventricular filling
- Normal left ventricular systolic function
- Etiology
- Primary/idiopathic
- Secondary (more common)
- Infiltrative disorders
- Amyloidosis
- Sarcoidosis
- Storage diseases
- Haemochromatosis
- Glycogen storage disease
- Endomyocardial fibrosis
- Systemic sclerosis
- Diabetes mellitus
- Chest radiation
- Cardiotoxic drugs
- Infiltrative disorders
- Causes “backward” heart failure
- Clinical features
- Dyspnoea
- Most common symptom
- Peripheral oedema
- Hepatomegaly
- Jugular venous distension
- Dyspnoea
- Diagnosis
- Echocardiography
- Best initial and confirmatory test
- Endomyocardial biopsy, chest x-ray, etc.
- To determine underlying cause
- Echocardiography
- Treatment
- Limited treatment is available; treatment is mostly palliative
- Definition
- Arrhythmogenic right ventricular cardiomyopathy (ARVC)
- Least common cardiomyopathy
- Idiopathic cause
- The right ventricular wall is replaced by fibrous tissue, which causes thinning and dilation of the right ventricle, which predisposes to ventricular arrhythmias and right ventricular dysfunction
- Clinical features
- Dizziness
- Palpitations
- Syncope
- Diagnosis
- Echocardiography
- Best initial and confirmatory test
- Endomyocardial biopsy
- Echocardiography
- Treatment
- Intense exercise is forbidden in all patients with ARVC
- Antiarrhythmic therapy
- Beta blockers (Sotalol)
- Amiodarone
- Screening of 1st-degree relatives
- Prevention of SCD
- No intense exercise
- Secondary prevention with ICD
- See topic 10
- Primary prevention with ICD
- In those at high risk for SCD
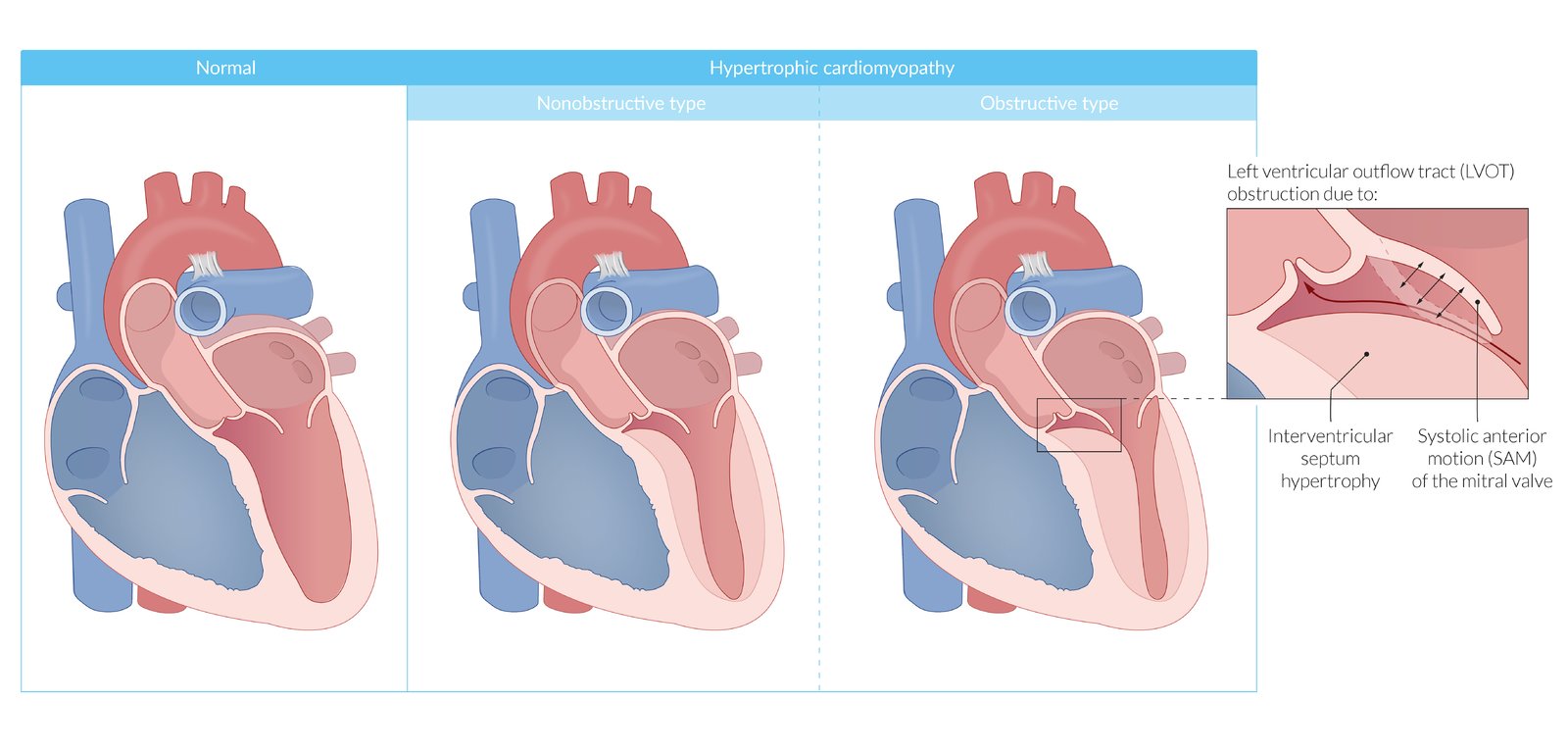{kind=link}
Other cardiomyopathies
- Tachycardia-induced cardiomyopathy (= tachycardiomyopathy)
- Cardiomyopathy (left ventricular dysfunction) caused by long-standing tachyarrhythmia (sustained ventricular rate of > 100 bpm)
- Has been reported with nearly all types of tachyarrhythmias
- Possible pathomechanisms
- Depletion of myocardial energy stores
- Abnormal calcium channel activity and calcium transport
- Abnormal beta-adrenergic receptor response
- Oxidative injury
- Clinical features
- Equal to those of heart failure
- Diagnosis
- Holter monitoring
- Sustained heart rate of > 100 bpm
- Exclusion of other causes of cardiomyopathy
- Holter monitoring
- Treatment
- Treatment of the underlying tachycardia
- Treatment of HFrEF
- Completely reversible in most cases
- Cardiomyopathy (left ventricular dysfunction) caused by long-standing tachyarrhythmia (sustained ventricular rate of > 100 bpm)
- Takotsubo cardiomyopathy
- Also called stress cardiomyopathy or apical ballooning syndrome
- Cardiomyopathy caused by physical or emotional stress
- Clinical features
- Often presents similarly to ACS
- Acute chest pain
- Dyspnoea
- Syncope
- Pathophysiology
- Stress -> catecholamine surge -> transient myocardial stunning
- Diagnosis
- ECG
- Features similar to those of ACS
- Echocardiography
- Shows characteristic “ballooning” of the left ventricular apex
- Coronary angiography
- Absence of obstructive coronary artery disease
- Small-to-intermediate increase in troponin
- The symptoms are often much greater than the increase in troponin would indicate, which can cause suspicion of takotsubo
- ECG
- Treatment
- Supportive therapy, if necessary
- Spontaneously resolves
- Ischaemic cardiomyopathy
- = refers to the impaired left ventricular function which occurs due to coronary artery disease
- Due to myocardial infarction, chronic myocardial ischaemia, etc.
- Technically not a cardiomyopathy, but the term is often used clinically anyway
- Myocardial infarction or recurrent ischaemia causes loss of myocardium, and ventricular remodelling
- Prognosis
- It’s reversible if it’s caused by recurrent ischaemia
- It’s not reversible if caused by myocardial infarction
- Treatment
- Same as for other heart failure and ischaemic heart disease patients
- Revascularization (CABG, PCI) if appropriate
- = refers to the impaired left ventricular function which occurs due to coronary artery disease
- Hypertensive cardiomyopathy
- = refers to the left ventricular hypertrophy which occurs due to systemic hypertension
- Technically not a cardiomyopathy, but the term is often used clinically anyway
- The hypertrophy predisposes to heart failure, ventricular arrhythmias, myocardial infarction, and sudden cardiac death
- Diagnosis
- Echocardiography
- ECG
- Prognosis
- Partly or completely reversible if the hypertension is treated
- Treatment
- Treatment of the underlying hypertension
- For peripartum cardiomyopathy, see topic 43
33. Myocarditis and rheumatic fever
- Myocarditis
- Occur more commonly in young adults
- Can be anywhere from acute and fulminant to chronic
- Etiology
- Viral
- Coxsackie B
- Parvovirus B19
- HHV6
- Bacterial
- Strep. pyogenes (rheumatic fever)
- Borreliosis
- Connective tissue diseases
- SLE
- Radiation
- Alcohol, cocaine
- Viral
- Clinical features
- Often asymptomatic
- Symptoms are highly variable
- The patient may have symptoms of a viral infection in the weeks before
- Acute myocarditis
- New onset or worsening heart failure
- ACS-like symptoms
- Arrhythmias
- Ventricular arrhythmias
- High grade AV block
- Chronic myocarditis
- Chest pain
- Palpitation
- Heart failure
- Diagnosis
- ACS in patients with no risk factors for CAD or if coronary angiography is negative should raise suspicion for myocarditis
- Endomyocardial biopsy
- Complications
- Cardiogenic shock
- Sudden cardiac death
- Viral myocarditis can progress into dilated cardiomyopathy
- Probably because anti-viral antibodies also attack the myocardium in some people
- Treatment
- Supportive treatment
- Treatment of symptoms (heart failure, arrhythmias)
- Treatment of underlying cause, if possible
- Antibiotics, immunosuppressive therapy (only in autoimmune etiology)
- Rheumatic fever
- = an acute inflammatory complication a few weeks after a strep. pyogenes pharyngitis
- The pharyngitis is subclinical in many cases, causing only approx. 50% of patients with rheumatic fever to recall having any upper respiratory symptoms lately
- Epidemiology
- Rare in developed countries
- Common in developing countries
- Pathomechanism
- Antibodies develop against the “M protein” of step. pyogenes
- These antibodies cross-react with nerves and myocardium due to molecular mimicry -> type II hypersensitivity reaction
- Clinical features
- Joint involvement
- Migratory polyarthritis
- Heart involvement (rheumatic heart disease)
- in 30 – 60% of cases
- Pancarditis (rheumatic carditis)
- Endocarditis, myocarditis, pericarditis
- Valvular involvement
- Mitral regurgitation/stenosis
- Rheumatic fever is the most common cause of mitral stenosis
- Aortic regurgitation/stenosis
- Mitral regurgitation/stenosis
- The heart involvement may cause arrhythmias or heart failure
- CNS involvement
- Skin involvement
- Joint involvement
- Diagnosis
- Echocardiography
- For valvular abnormalities
- Based on the JONES criteria and clinical features
- Echocardiography
- Treatment
- Oral penicillin V
- NSAIDs
- Treatment of heart failure or arrhythmias
- Rheumatic heart disease is only reversible is ~50% of cases
- The remainder develop chronic rheumatic heart disease
- Development of heart failure, stroke and endocarditis is common in people with rheumatic heart disease
- In some patients the rheumatic fever itself is subclinical, causing some patients to present with rheumatic heart disease years after the rheumatic fever
- Joint, CNS and skin involvement are reversible
- Secondary prevention
- Those who already have had rheumatic fever are predisposed to recurrence of it later
- Recurrence increases the risk for developing chronic rheumatic heart disease or worsening of it
- Secondary prevention by giving IM penicillin for many years is indicated in all patients with rheumatic fever
- = an acute inflammatory complication a few weeks after a strep. pyogenes pharyngitis
34. The diseases of the pericardium, cardiac tamponade
- Acute pericarditis
- Can be isolated or with myocarditis
- Can be fibrinous or serous
- Etiology
- Most cases idiopathic
- Viral (esp. Coxackie B)
- Myocardial infarction
- Either within a few days (post-infarction fibrinous pericarditis)
- or after weeks/months (postmyocardial infarction syndrome/Dressler syndrome)
- Post-pericardiotomy syndrome
- Pericarditis after injury to the pericardium during surgery
- SLE, RA
- Uraemia
- Radiation
- Clinical features
- Fever
- Dyspnoea
- Dry cough
- Chest pain
- Sharp, “pleuritic”
- Improves when sitting and leaning forward
- Worsens when coughing, swallowing, inspiring
- Pericardial friction rub
- High-pitched scratching sound
- Heard at left sternal border
- During expiration, when patient is sitting up and leaning forward
- Pericardial effusion
- Diagnosis
- Labs
- Leukocytosis
- ESR, CRP elevated
- ECG
- Follows 4 stages (only first stage is important I think)
- Stage 1
- ST elevation in almost all leads
- ST depression in aVR, V1
- PR depression in some leads
- Stage 2
- ST abnormalities normalize after 1 week
- Stage 3
- Inverted T-waves
- Stage 4
- ECG normalizes after weeks
- Echocardiography
- Might show effusion
- Chest X-ray normal
- Labs
- Treatment
- Treat underlying cause, if any
- NSAIDs
- Colchicine
- If idiopathic
- Complications
- Constrictive pericarditis
- A complication of acute fibrinous pericarditis
- The pericardium becomes fibrotic, which compromises cardiac filling
- Cardiac tamponade
- A complication of acute serous pericarditis if rapid pericardial effusion develops
- Constrictive pericarditis
- Constrictive pericarditis
- Clinical features
- Symptoms of forward failure
- Tachycardia
- Dyspnoea
- Pericardial knock
- Sound of the sudden cessation of ventricular filling during diastole
- Heard best at left sternal border
- Pulsus paradoxus
- Symptoms of backward failure
- Jugular vein distension
- Kussmaul sign
- Jugular vein distends during inspiration
- Hepatomegaly
- Peripheral oedema
- Ascites
- Symptoms of forward failure
- Diagnosis
- Chest X-ray
- Pericardial thickening and calcifications
- Echocardiography
- Pericardial thickening
- Ventricular filling suddenly halts during diastole
- ECG normal
- Chest X-ray
- Treatment
- Treat underlying cause
- Pericardiectomy
- Clinical features
- Pericardial effusion and cardiac tamponade
- Pericardial effusion
- = Accumulation of fluid in pericardial space
- Serous fluid – due to pericarditis
- Blood (haemopericardium)
- Cardiac wall rupture
- Aortic dissection
- Pericardial effusion itself is asymptomatic, and requires no treatment, but it can cause cardiac tamponade
- Cardiac tamponade
- = A compression of the heart due to rapid pericardial effusion
- An emergency with characteristic clinical features
- The size of the pericardial effusion is not the most important,
- Rather, the speed at which the effusion develops determines whether the heart function will be compromised or not
- Clinical features
- Beck triad
- Hypotension
- Jugular venous congestion
- Weak heart sounds
- Tachycardia
- Pulsus paradoxus
- Dyspnoea
- Worsens when lying down
- Improves when sitting
- Beck triad
- Diagnosis
- Echocardiography
- Gold standard for tamponade diagnosis
- Can detect even small amounts of pericardial effusion
- Anechoic pericardial space + reduced wall motion and EF
- ECG
- Electric alternans
- Consecutive QRS complexes alternate in height
- Low voltage
- Electric alternans
- Chest X-ray
- Enlarged heart
- Water bottle-shaped heart
- Echocardiography
- Treatment
- Immediate US-guided pericardiocentesis
- Supportive therapy
- Pericardial effusion
35. Infective endocarditis (IE)
- Due to possibility for extracardiac complications, a multidisciplinary team is often needed
- Risk factors
- Pre-existing conditions
- Artificial heart valve
- Damaged heart valve
- Congenital heart defect
- Immunosuppression
- Bacteraemia
- IV drug abuse
- Infected indwelling catheters
- Dentistry procedures
- Surgery
- Pre-existing conditions
- Acute bacterial endocarditis
- S. aureus, S. pneumoniae
- Rapid progression (days)
- More severe symptoms
- More common in artificial valves
- Subacute bacterial endocarditis
- S. viridans
- Slow progression (weeks, months)
- Less severe symptoms
- More common in native valves
- Pathomechanism
- Intact endothelium is resistant to bacteraemia -> endothelial damage must be present for bacteria to colonize
- Results of bacterial colonization
- Bacterial colonization of valves destroys the valve
- Bacterial vegetations loosen and embolize -> infarction of brain, spleen, kidney, etc.
- Immune complexes and antibodies against bacteria deposit -> glomerulonephritis, Osler nodes, etc.
- Clinical features
- Fever (of unknown origin)
- Tachycardia
- Malaise
- New or changed heart murmur
- Heart failure
- Can be acute or slowly progressive
- Roth spots (retinal haemorrhages with pale middle)
- Osler nodes (painful subcutaneous nodules on fingers, toes)
- Janeway lesions (non-painful, erythematous macules on palms, soles)
- Subuncal haemorrhage
- Haemorrhages under fingernails
- Glomerulonephritis
- Haematuria
- Renal failure
- Neurological symptoms
- Due to so-called “mycotic aneurysms” in the brain which rupture
- Bacterial emboli embolize vasa vasorum of cerebral arteries, causing these aneurysms
- Diagnosis
- Duke criteria
- There are major and minor criteria
- The presence of any of the following combinations of positive criteria confirms endocarditis:
- 2 major criteria + 0 minor criteria
- 1 major criteria + 3 minor criteria
- 0 major criteria + 5 minor criteria
- Major criteria
- Blood cultures show typical organism
- Echocardiographic evidence of endocarditis
- New murmur
- Minor criteria
- Predisposing risk factors (especially IV drug use)
- Fever
- Vascular abnormalities
- Emboli, intracerebral haemorrhage, etc.
- Immunological abnormalities
- Glomerulonephritis, Osler nodes, Roth spots, etc.
- Blood cultures show atypical organism
- Blood culture
- 3 sets must be taken with 30 minutes in-between (at 0, 30, 60 minutes)
- Preferably before initiation of empiric treatment
- Blood culture-negative IE (BCNIE)
- = IE where no causative bacteria can be grown on normal blood culture methods
- 5 – 10% of all IE cases
- Can be due to
- Prior antibiotic therapy
- Microorganisms which don’t grow on normal blood cultures (fungi, protozoa)
- PCR is used to detect the microorganisms instead
- Echocardiography
- Can show vegetations, dysfunctional valves, abscesses, etc.
- Initially transthoracic
- -> if positive findings -> transoesophageal
- -> if negative but high suspicion for IE -> transoesophageal
- If artificial valve -> initial transoesophageal
- Labs
- Leukocytosis
- ESR, CRP elevated
- Duke criteria
- Treatment
- Empirical antibiotic therapy
- Preferably after blood culture samples are taken
- Bactericidal rather than bacteriostatic antibiotics are used
- As the immune system can’t reach the vegetations, bacteriostatic antibiotics are less useful
- Exact drug depends on risk factors
- Vanco + genta is appropriate for many cases
- Targeted antibiotic therapy
- After the infectious agent and the AB sensitivity is determined
- Can last many weeks (often 2 – 6)
- Surgical
- Indicated if there is acute heart failure or uncontrolled infection
- Vegetations are removed, area is cleaned, valve may be replaced
- Empirical antibiotic therapy
- Prophylaxis
- Primary
- Good oral hygiene
- No piercing, tattoos
- Secondary
- Before high-risk procedures
- Amoxicillin is preferred
- For patients who:
- Had previous infective endocarditis
- Have unrepaired cyanotic congenital heart disease
- Have any artificial material in their heart
- For the following procedures:
- Dental work involved gingiva or mucosa
- Endoscopy or surgery involving infected areas, abscesses
- etc.
- Primary
36. Diseases of the mitral valve
- Mitral regurgitation (MR)
- Primary mitral regurgitation
- = MR due to conditions that affect the mitral valve itself
- Rheumatic fever
- Mitral valve prolapse
- Connective tissue diseases
- Secondary (functional) mitral regurgitation
- = MR due to conditions that affect the papillary muscle or left ventricle
- Myocardial infarction (ischaemic cardiomyopathy)
- Dilated cardiomyopathy
- Pathophysiology
- MR causes volume and pressure load on the left atrium
- Acute: -> increased pressure in pulmonary veins -> pulmonary oedema
- Chronic: -> dilation of left ventricle
- Mitral regurgitation also decreases stroke volume ->
- Acute: -> decreased CO, forward heart failure
- Chronic: -> left ventricular hypertrophy and dilation to compensate
- MR causes volume and pressure load on the left atrium
- Can be acute or chronic
- Acute mitral regurgitation causes acute left-sided heart failure with pulmonary oedema
- Chronic mitral regurgitation causes palpitations and dyspnoea
- Diagnosis
- Holosystolic murmur (can be heard throughout the systole as blood is regurgitated)
- Radiates to axillary region
- ECG
- Left ventricular hypertrophy
- P mitrale
- Echocardiography
- Gold standard
- Holosystolic murmur (can be heard throughout the systole as blood is regurgitated)
- Treatment
- Acute mitral regurgitation
- Haemodynamic stabilization
- Urgent surgical valve repair or replacement
- Chronic mitral regurgitation
- Surgical valve repair or replacement
- Acute mitral regurgitation
- Primary mitral regurgitation
- Mitral stenosis
- Etiology
- Rheumatic fever
- Accounts for almost all cases
- SLE
- Rheumatic fever
- Pathophysiology
- Decreased blood flow into the left ventricle -> decreased stroke volume -> forward heart failure
- Increased pressure load on the left ventricle -> increased pressure in pulmonary circulation -> pulmonary oedema
- Situations which increase CO or cause tachycardia increase the pulmonary congestion, worsening symptoms
- Clinical features
- Patients usually progress from asymptomatic to symptoms during exertion to symptoms during rest
- Dyspnoea
- Most common, and often the only symptom
- Haemoptysis
- Diagnosis
- Diastolic murmur
- Loud first heart sound (S1)
- ECG
- P mitrale
- Echocardiography
- Gold standard
- May be performed with exercise if nothing is found during rest
- Treatment
- Asymptomatic and low grade
- Treatment of heart failure or atrial fibrillation
- High grade or symptomatic mitral stenosis
- Percutaneous mitral commissurotomy (PMC)
- First line
- Open commissurotomy or surgical valve replacement
- Percutaneous mitral commissurotomy (PMC)
- Asymptomatic and low grade
- Complications
- Atrial fibrillation
- Due to dilation of left atrium
- Atrial fibrillation can worsen symptoms, as normal atrial contraction is important to maintain transmitral blood flow in case of mitral stenosis
- Heart failure
- Atrial fibrillation
- Etiology
37. Diseases of the aortic valve
- Aortic regurgitation (AR)
- Acute AR
- Infective endocarditis
- Stanford type A aortic dissection
- Chronic AR
- Congenital bicuspid valve
- Rheumatic heart disease
- Pathophysiology
- Blood flows back into the LV after systole
- -> Increased end-diastolic volume in left ventricle -> increased contraction -> increased systolic blood pressure
- -> decreased diastolic blood pressure
- Acute AR
- Regurgitant blood causes backward congestion into the pulmonary circulation
- Chronic AR
- Increased volume load on the left ventricle causes LV hypertrophy and remodelling -> LV dysfunction
- Blood flows back into the LV after systole
- Clinical features
- Acute AR
- Sudden onset symptoms
- Dyspnoea
- Pulmonary oedema
- Acute heart failure
- Chronic AR
- May be asymptomatic for long
- Palpitations
- Symptoms of left heart failure
- Symptoms of high pulse pressure
- Head pounding
- Bobbing of heat in synchrony with heartbeats
- Acute AR
- Diagnosis
- High systolic but low diastolic BP
- Third heart sound (S3)
- Early diastolic murmur
- As blood regurgitates into LV
- Echocardiography
- Gold standard
- Treatment
- Conservative
- For asymptomatic patients, or symptomatic patients who are not candidates for surgery
- Treatment of heart failure
- Surgical
- Valve repair or valve replacement
- For patients with symptoms or LV dysfunction, or with severe AR
- Conservative
- Acute AR
- Aortic stenosis (AS)
- Epidemiology
- Most common valvular disease
- Calcific aortic stenosis is a common progressive dystrophic calcification and degeneration of the aortic valve
- It affects more than 65% of elderly
- Etiology
- Congenital (Bicuspid aortic valve)
- Acquired (Calcific aortic stenosis)
- Pathophysiology
- Bicuspid aortic valve predisposes the valve to dystrophic calcification and degeneration, causing aortic stenosis to occur early
- Aortic stenosis causes increased pressure load on LV:
- -> LV hypertrophy and remodelling -> LV dysfunction
- -> Increased LV oxygen demand -> increased risk for angina, infarction
- Clinical features
- Patients usually progress from asymptomatic to symptoms during exertion to symptoms during rest
- Dyspnoea
- Angina pectoris
- Syncope
- Diagnosis
- Loud systolic murmur
- Radiates to carotids
- Crescendo-decrescendo
- At right second intercostal space
- Pulsus parvus et tardus (weak and delayed pulse)
- Echocardiography
- Gold standard
- Loud systolic murmur
- Treatment
- Conservative
- For asymptomatic patients with mild stenosis
- Treatment of heart failure
- Regular follow-up
- Surgical
- For patients with symptoms or severe stenosis
- Surgical aortic valve replacement (SAVR)
- Transcatheter aortic valve implantation (TAVI)
- For those with high surgical risk
- Conservative
- Epidemiology
38. Combined and multiple valve diseases
- Combined valve disease
- Refers to stenosis and regurgitation on the same valve
- Combination of stenosis and regurgitation is considered severe even though the stenosis and regurgitation are themselves of only mild severity
- Epidemiology
- Most commonly aortic stenosis and regurgitation
- Etiology
- Congenital heart disease
- Rheumatic heart disease
- Degenerative heart disease
- Multiple valve diseases
- Refers to the presence of multiple diseased valves in same patient
- Epidemiology
- Most commonly the aortic and mitral
- Not as rare as you’d think – around 10 – 20% of patients with valvular heart disease have multiple diseased valves
- Etiology
- Rheumatic heart disease
- Degenerative valvular heart disease
- Congenital heart diseases
- Infective endocarditis
- The management of multiple valve disease is dictated by the predominant valvular disease
- The presence of multiple diseased valves may mask the severity of the individual valvular diseases
- For example, mitral regurgitation leads to the underestimation of the severity of aortic stenosis
39. Pulmonary embolism and primary pulmonary hypertension
- Pulmonary embolism (PE)
- The risk factors for pulmonary embolism are the same as the risk factors for deep vein thrombosis
- Obesity
- Immobility
- Cancer
- Pregnancy
- Hypercoagulability
- Previous DVT
- (see also surgery 1 topic 8)
- Pathophysiology
- Infarction of lung and pleura
- Ventilation-perfusion mismatch
- Due to the ventilated alveoli with blocked vessels
- Increased pulmonary artery pressure
- -> forward failure
- Clinical features
- Can range from asymptomatic to sudden death
- Dyspnoea
- Most common symptom
- Tachypnoea
- Chest pain
- Often pleuritic
- Cough
- Symptoms of DVT
- Haemoptysis
- Wells criteria for pulmonary embolism
- Scoring system which determines the pre-test probability for PE
- Parameters
- Clinical symptoms of DVT – 3 points
- PE more likely than other diagnoses – 3 points
- Heart rate > 100 – 1,5 points
- Immobilization or surgery recently – 1,5 points
- Previous DVT/PE – 1,5 points
- Haemoptysis – 1,0 points
- Malignancy – 1,0 points
- Probability
- Traditional Wells criteria
- Score 0 – 2 – low probability
- Score 2 – 6 – moderate probability
- Score > 6 – high probability
- Simplified (modified) Wells criteria
- Score < 4 – PE unlikely
- Score > 4 – PE likely
- Traditional Wells criteria
- Diagnosis
- Patients with suspected PE and haemodynamic instability
- Echocardiography
- If no RV dysfunction -> PE excluded
- If RV dysfunction -> CTPA
- Echocardiography
- Patients with low or moderate pre-test probability for PE (Wells 0 – 6)
- D-dimer
- Positive -> CTPA
- Negative -> PE excluded
- D-dimer
- Patients with high pre-test probability for PE (Wells > 6)
- CTPA
- Lab
- CBC
- Liver and kidney function
- Kidney function is important in case contrast is needed for CT angiography
- Arterial blood gas
- Hypoxaemia is common
- D-dimer
- High negative predictive value for PE
- No positive predictive value for PE
- Imaging techniques
- CTPA
- Best imaging technique
- Alternatives
- V/Q scan
- Pulmonary angiography
- CTPA
- Patients with suspected PE and haemodynamic instability
- Treatment
- Patients with PE and haemodynamic instability
- Stabilization with fluids, vasopressors, etc.
- Anticoagulation should be initiated immediately, even before definitive diagnosis has been made, as long as there are no contraindications to anticoagulation
- Systemic thrombolysis is indicated
- Patients with high pre-test probability for PE
- Anticoagulation should be initiated immediately, even before definitive diagnosis has been made, as long as there are no contraindications to anticoagulation
- Patients with moderate pre-test probability for PE
- Anticoagulation should be initiated immediately, even before definitive diagnosis has been made, as long as there are no contraindications to anticoagulation
- Patients with low pre-test probability for PE
- Anticoagulation is started after the diagnosis is confirmed
- Anticoagulation
- With LMWH or UFH
- Thrombolytic therapy
- With a tPA like alteplase
- Embolectomy
- If thrombolytic therapy fails or is contraindicated
- Can be performed surgically or with catheter
- IVC filter
- A filter, placed endovascularly into the IVC
- The filter traps emboli on the way to the lungs
- Used if PE is confirmed in patients who have contraindications to anticoagulation
- Patients with PE and haemodynamic instability
- Complications
- Recurrent thromboembolism is common in patients who have had PE
- See secondary prevention
- Chronic thromboembolic pulmonary hypertension
- Refers to pulmonary hypertension developing as a late complication of PE
- Affects 25% of patients with PE
- Death
- The mortality of untreated PE is 30%
- The mortality of treated PE is under 10%
- Most cases of death occur within the first week after the first PE
- Death occurs due to recurrent thromboembolism and shock
- The mortality of untreated PE is 30%
- Recurrent thromboembolism is common in patients who have had PE
- Secondary prevention
- Prevention of recurrence
- Secondary prevention is a simple continuance of the anticoagulation which was started in the hospital
- With LMWH, NOAC or warfarin
- Duration of anticoagulation
- Anticoagulation should last for at least 3 months for all patients with PE
- For patients with their first PE/DVT, or those with PE secondary to a major transient risk factor, the anticoagulation can be stopped after 3 months
- For patients with recurrent PE/DVT, the anticoagulation should last indefinitely
- The risk factors for pulmonary embolism are the same as the risk factors for deep vein thrombosis
- Idiopathic pulmonary arterial hypertension (IPAH) (Primary pulmonary hypertension)
- Refers to pulmonary arterial hypertension without specific cause
- Pathophysiology
- For unknown reasons small pulmonary arteries and arterioles are obliterated
- This gradually increases the pulmonary vascular resistance
- Clinical features
- Exertional dyspnoea and fatigue
- Diagnosis
- Echocardiography
- Right heart catheterization
- Necessary for definite diagnosis
- Increased mean pulmonary arterial pressure (mPAP > 20 mmHg)
- Increased pulmonary vascular resistance (PVR > 3 Wood units)
- Treatment
- Diuretics
- Prostanoids
- Endothelin receptor antagonists
- IP receptor antagonists
- PDE inhibitors
- Sildenafil
- CCBs
- Some cases of IPAH respond to CCBs
- Prognosis
- Median survival 3 years without treatment
40. Anticoagulant and fibrinolytic therapy in cardiovascular diseases + 41. Antiplatelet therapy in cardiovascular diseases
- Anticoagulant and antiplatelet therapy
- Anticoagulant therapy refers to the use of UFH, direct thrombin inhibitors, LMWH, NOACs or vitamin K antagonists
- Antiplatelet therapy refers to the use of aspirin, P2Y12 inhibitors or GP IIb/IIIa antagonists
- For the P2Y12 inhibitors, clopidogrel is generally considered inferior to prasugrel or ticagrelor
- Dual antiplatelet therapy (DAPT) refers to the concomitant use of aspirin and a P2Y12 inhibitor
- Doses
- Aspirin
- Loading dose – 300 mg
- Daily dose – 100 mg
- Clopidogrel
- Loading dose – 600 mg
- Every (normal) tablet of clopidogrel is 75 mg, so that’s 8 tablets!
- 300 mg tablets also exist
- Daily dose – 75 mg
- Loading dose – 600 mg
- Ticagrelor
- Loading dose – 180 mg
- Aspirin
- In acute coronary syndrome
- Patients presenting with ACS should receive dual antiplatelet therapy at FMC, in the form of loading dose aspirin and loading dose clopidogrel or ticagrelor
- In most cases, these patients will undergo PCI and therefore remain on DAPT for 1 year
- Patients presenting with ACS should also receive anticoagulation therapy at FMC, in the form of UFH or LMWH
- Anticoagulant therapy is stopped after PCI unless another indication for anticoagulation remains
- Patients who have experienced ACS should receive aspirin for life
- Patients presenting with ACS should receive dual antiplatelet therapy at FMC, in the form of loading dose aspirin and loading dose clopidogrel or ticagrelor
- In atrial fibrillation
- In non-valvular atrial fibrillation
- Lifelong anticoagulation is indicated for patients with non-valvular atrial fibrillation and CHA₂DS₂-VASc score 2 or more
- NOACs or warfarin
- In valvular atrial fibrillation
- Lifelong anticoagulation is indicated for all patients with valvular atrial fibrillation, regardless of CHA₂DS₂-VASc score
- Warfarin only
- In non-valvular atrial fibrillation
- In prosthetic heart valves
- For mechanical valves
- Life-long anticoagulation with warfarin
- Aspirin may be added as well
- For biological valves
- Warfarin for only 3 months
- For mechanical valves
- In pulmonary embolism
- Anticoagulation during the PE and for at least 3 months after
- PCI
- All patients undergoing PCI should be on both DAPT and anticoagulation
- All patients who have undergone PCI should receive DAPT for 1 year, followed by lifelong aspirin
- Fibrinolytic therapy
- Fibrinolytic (or thrombolytic) therapy refers to using tissue plasminogen activators (tPA) like alteplase, or other agents like urokinase
- In ACS with STEMI
- Fibrinolytic therapy is indicated in STEMI if the patient cannot be transported to a PCI lab within 2 hours
- Fibrinolytic therapy is never indicated in NSTEMI or unstable angina
- In pulmonary embolism with haemodynamic instability
- In acute ischaemic stroke
42. Laboratory diagnostics in cardiology, biomarkers
- (Cardiac) Troponin (cTn)
- Two subtypes exist, troponin T and troponin I
- There is no significant difference between the types. Both can be used
- Normal value of troponin T is < 14 ng/L
- Normal value of troponin I is < 0,4 ng/mL
- Troponins can be elevated in many other cardiac and non-cardiac diseases
- Myocarditis, heart failure, arrhythmia, trauma, kidney failure
- However, in these diseases the troponins are often elevated but stable
- For troponins to be specific for myocardial infarction we must demonstrate a so-called rise and/or fall
- This means that we must take multiple (at least 2) blood samples at two different times after admission, and that these samples show that the patient’s troponin level is either rising and/or falling, over time
- This is because troponin is released as the myocardium is necrotic. As more and more myocardium become necrotic, a rise in troponin occurs
- See figure 7 here
- The degree of elevation of troponins correlates with the size of the infarct
- Troponins are elevated 3 – 4 hours after the onset of infarction
- They reach the max after 12 – 24 hours
- Troponins are normalized 7 – 10 days after the onset of infarction
- This means that troponins cannot be used to evaluate a reinfarction which occurs within 7 – 10 days
- Two subtypes exist, troponin T and troponin I
- CK-MB (creatine kinase-muscle/brain)
- CK-MB is more specific to myocardium than total CK
- Not commonly used
- Can be helpful for evaluating reinfarction which occurs after a few days
- This is because CK-MB has a short half-life. Its level normalizes after 2 – 3 days
- This means that the CK-MB elevation from the first infarction will be normalized before the second infarction occurs (as long as it occurs more than 2 – 3 days after the first)
- Natriuretic peptides
- The natriuretic peptide BNP and its inactive fragment NT-proBNP are excellent markers of heart failure
- More specifically, these markers are increased in response to increased load on the left ventricle
- The degree of increase is proportional to the increased load
- NT-proBNP is more commonly measured than BNP
- The physiological effect of BNP is to stimulate natriuresis and urine production in the kidney, decreasing preload
- The peptides are released renally, so they’re increased in renal failure
- Uses
- To follow up treatment response in patients with HF
- To increase the likelihood of HF as a diagnosis
- High NT-proBNP increases the likelihood of HF
- The higher the value, the higher the likelihood
- To exclude HF as a diagnosis
- NT-proBNP has good negative prognostic value
- To evaluate the prognosis of HF
- Higher NT-proBNP is associated with worse prognosis
- The natriuretic peptide BNP and its inactive fragment NT-proBNP are excellent markers of heart failure
- Important laboratory parameters in cardiology
- Glucose
- HBA1c
- Lipid panel
- Total cholesterol, triglycerides, HDL, LDL
- Kidney function (Creatinine, eGFR)
- To determine viability for contrast agents and certain medications
- CBC
- Evaluate anaemia
- Artificial valvular leak can cause haemolysis
- CRP
- For infective endocarditis, pericarditis, myocarditis
- Liver function
- To look for side effects of statins
- Liver failure can cause peripheral oedema, like HF
- Electrolytes
- Important to monitor in case of HF, and diuretic treatment
- INR
- To monitor VKAs
- TSH
- Thyroid dysfunction can cause HF, AF, etc.
- D-dimer
- Pulmonary embolism
43. Pregnancy and heart disease
- Many physiological, especially haemodynamical, changes occur during pregnancy which can precipitate or worsen heart disease
- Cardiovascular diseases during pregnancy are the most common causes of pregnancy-associated mortality
- Women of childbearing age with heart disease should undergo risk stratification, to evaluate the risk of unwanted events in case of pregnancy
- The mWHO classification of maternal cardiovascular risk is used
- Those at highest risk (mWHO class IV) should be recommended against pregnancy, at least until the risk is treated (if possible)
- Contraception and possible termination of pregnancy is recommended
- Pulmonary arterial hypertension
- NYHA III or IV
- Severe aortic dilatation
- Significant valvular stenosis
- Peripartum cardiomyopathy
- = the development of systolic heart failure towards the end of pregnancy or in the months following it
- Unknown etiology
- Clinical features like those of systolic heart failure
- Treated like normal heart failure, except for ACEis and ARBs
- 50 % normalize after delivery
- Anticoagulation
- LMWHs or UFH are preferred
- Biological rather than mechanical valves are recommended in young women contemplating pregnancy
- Due to the decreased duration of anticoagulative therapy
- Arrhythmias
- Atrial fibrillation should be electrically cardioverted rather than rhythm controlled
- Cardiovascular drugs contraindicated in pregnancy
- VKAs
- Can be used from the 2nd trimester up until the 36th week
- Amiodarone
- ACEIs
- ARBs
- VKAs
44. Cardiac rehabilitation
- Cardiac rehabilitation is a program of activities and interventions which aim to ensure the best possible physical, mental and social conditions for patients with chronic or post-acute cardiovascular disease
- Cardiac rehabilitation is also important in secondary prevention
- Participation in cardiac rehabilitation reduces three-year mortality by 25%
- Cardiac rehabilitation is underused
- Only 1/3 of eligible patients are referred to it
- Only 11% of eligible patients adhere to it
- Phases
- Inpatient phase
- Rehabilitation begins while the patient is in the hospital
- Outpatient phase
- After discharge the patient will attend outpatient rehabilitation clinics and programs
- Lasts 4 – 12 weeks
- Maintenance phase
- During the maintenance phase the patient themselves will be responsible for maintaining the habits they’ve learned
- Patient will have infrequent regular checkups
- Inpatient phase
- Indications
- Coronary artery disease
- Previous AMI
- After CABG, PCI
- Patients with stable CAD
- Heart failure
- Medically treated stable patients with NYHA II or III
- Surgically treated heart failure patients
- Post heart transplantation
- Post valvular surgery
- Post PM/ICD implantation
- Coronary artery disease
- Components
- Regular physical exercise
- Dietary counselling
- Smoking cessation
- Adherence to and optimization of medical therapies mentioned in topic 22
- Patient education
- Goals
- Achieve greater physical exercise capacity
- Improve risk profile and reduce future CV events
- Improve quality of life
- Improve social functioning
- Prevent hospital admissions
- Improve patient survival
45. The role of multicentre, international clinical studies in the therapy of heart diseases (arrhythmias, ACS, secondary prevention, etc.)
- Multicentre, international clinical studies are necessary because often, our intuition may be wrong
- By performing the studies across multiple centres and ideally across multiple countries, we eliminate many biases and sources of errors
- The CAST (cardiac arrhythmia suppression trial, 1991) revealed that usage of class I antiarrhythmics after AMI increased mortality, rather than reduce it
- The drugs reduced the amount of VES but increased the amount of other, worse arrhythmias
- Because treating AMI patients with class I antiarrhythmics was standard at the time, many patients died unnecessarily
- Scientific guidelines often grade and classify their recommendations
- Grading of the evidence that underlies the recommendation is denoted by letters A, B and C
- Grade A refers to a recommendation which is the result of many randomized clinical trials
- Grade B refers to a recommendation which is the result of one randomized trial, or multiple nonrandomized trials
- Grade C refers to a recommendation which is based on expert consensus, without good clinical trials
- Classification of the recommendation is denoted by roman numbers I, IIa, IIb or III
- A class I recommendation is one where the procedure or treatment is recommended, as the evidence shows that the procedure or treatment is clearly beneficial
- A class IIa recommendation is one where the procedure or treatment should be considered, as the evidence shows that the procedure or treatment is beneficial in most cases
- A class IIb recommendation is one where the procedure or treatment may be considered, as the evidence shows that the procedure or treatment is beneficial in some cases
- A class III recommendation is one where the procedure or treatment is not recommended, as the evidence shows that the procedure or treatment is ineffective or harmful
- For example:
- A class I grade A recommendation is a strong recommendation based on high-quality evidence
- The choice of primary PCI vs fibrinolysis is a class I grade A recommendation
- A class IIa grade C recommendation is a moderate recommendation based on poor-quality evidence
- The choice of CABG in patients with STEMI who cannot undergo PCI is a class IIa grade C recommendation
- A class III grade B recommendation is a strong contraindication, based on moderate-quality evidence
- Beta blockers should be avoided in STEMI patients with concomitant hypotension, acute HF, AV block or severe bradycardia (a class III grade B recommendation)
- A class I grade A recommendation is a strong recommendation based on high-quality evidence
- Grading of the evidence that underlies the recommendation is denoted by letters A, B and C