So I had my A&IC exam today. It was a bit of an experience, especially an unexpected one. I’d heard that the exam is with no prep time and just 5 minutes, but the exams today were with preparation time and they took much longer than 5 minutes.
I’m not sure who the examiner was, but after looking at the department site I think it was Dr. Tamás Kiss. I don’t know who the co-examiner was.
Me and two Hungarian students enter the K001 seminar room at 400 bed clinic at 9:00, and we’re told to sit down with some distance. They ask who wants to start, and we agree amongst ourselves that I should start. I draw two topics from separate envelopes. I get:
- 14. Mental disorders, drug overdosed patients (the unconscious patient and toxins)
- 4. Pharmacology of inhalational anaesthetics
I expected to start the exam right away, but instead they gave me the paper to start preparing, which was a surprise. I hadn’t even brought a pen because I thought there wouldn’t be prep time. Anyway, I start preparing.
Even though I started preparing first, one of the other student finished before me, and so started the exam first. Their exam was in Hungarian, so I couldn’t understand much of what they were saying. From what I gathered, he was talking about monitoring during anaesthesia, and there were some things he’d forgotten to mention and the examiner spent A LOT of time helping him remember them. I think his exam lasted around 40 minutes. During this time I was thinking of how different this exam is going to be from my expectations.
After a while it’s my turn. I begin with my first topic.
14. Mental disorders, drug overdosed patients (the unconscious patient and toxins)
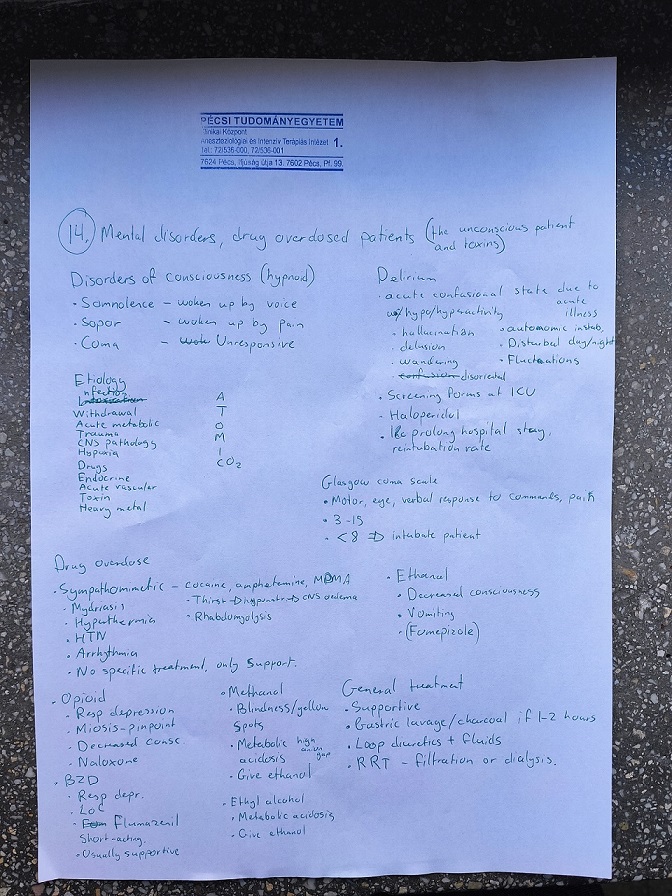
I began by saying that I can talk about the disorders of consciousness, to which he agreed. I mention the three types. Then I talk about the I WATCH DEATH mnemonic, which I’m not sure I remembered correctly but I didn’t make any comments about it. I also talked about the GCS. He then asked me about a simpler way to scale the patient’s consciousness. I barely remembered (after some help) about AVPU, and he asked me what it stands for. I barely remembered that as well.
I say that I can talk a bit about delirium here as well, which he agrees to. He mention what I’d written down. He asks me about what can cause delirium in the ICU specifically, as opposed to other hospital wards. I guess lots of things, like infection, sepsis, shock, postop, etc., but he says he’s after “something much simpler”. “Think about the typical patient. Who are they?” I say “elderly”, and he’s like “yes! exactly, simply old age and dementia can cause it”. Then he’s after another thing as well. Eventually he tells me “What’s different in the ICU compared to other wards? What happens at 2 in the night in the ICU?”, at which point I understand that he was talking about sleep deprivation, which was correct. He says to move on to the next part, the drugs.
I begin with the sympathomimetics, and before I can mention the symptoms he asks me what the symptoms are. He then tells me to talk about opioids, and I mention what I’d written. He asks me about the respiratory pattern in opioid intoxication. I mention that it is very slow and shallow, which he degrees with. He says that it’s deep rather than shallow.
At this point he says he’s happy and that we should move on to the next topic. I never covered the other drugs.
Pharmacology of inhalational anaesthetics
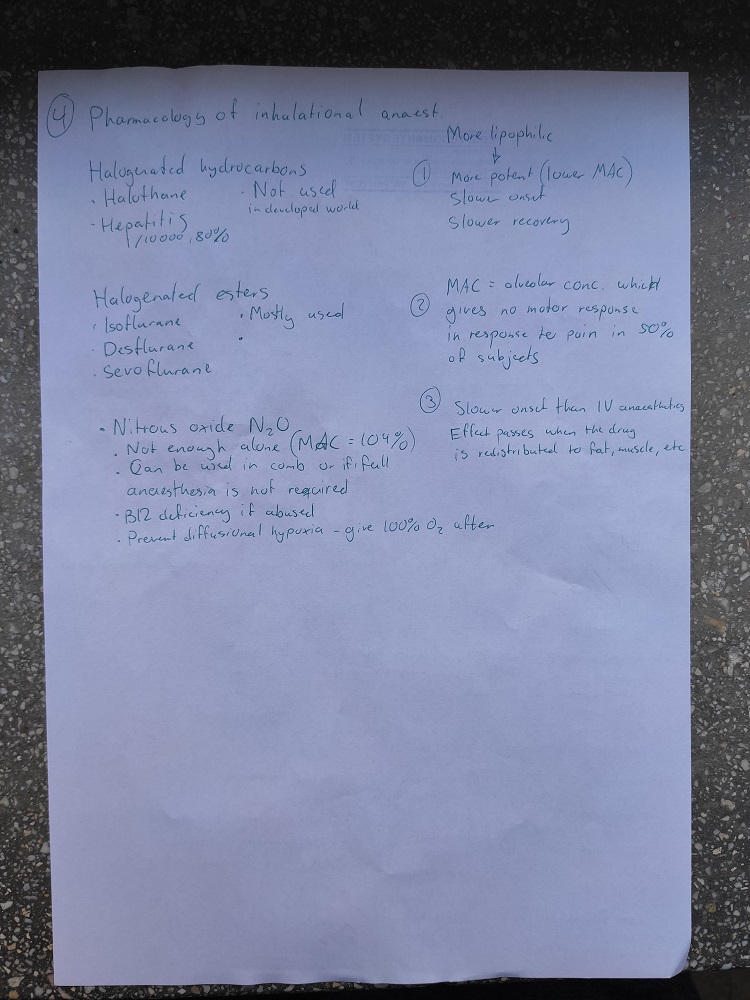
I begin by mentioning that inhaled anaesthetics are lipophilic drugs, and the more lipophilic, the more potent, the slower the onset, and the slower the recovery. I tell him the definition of MAC, after which he stops me and tells me that MAC isn’t really a measure of potency, for some reason he explains to me which I don’t really understand. He then asks which alveolar concentration of anaesthetic we use in general anaesthesia, to which I reply “1,3 x MAC”. He say’s “1,2 – 1,3, correct”.
I then mention point 3, before I talk about halothane. I mention what I’d written, and I continue to the halogenated ethers. I didn’t remember any of the specific effects of them during prep, so I hadn’t written any down as you can see. I continue to nitrous oxide, and mention what I’d written. He asks me about which other effect N2O has, aside from the anaesthesia itself. I guess “analgesia”, which was apparently correct.
He asks about situations where we could use it in alone. I mention procedures like dental procedures or colonoscopies, but they weren’t really what he was after. He says “in which situation do you think it’s an advantage that the patient does not completely lose consciousness, but is pain relieved? Think of younger women”, at which point I guess “during labour”, which was correct.
He then circles back to halogenated esters, probably because they’re the most widely used but I didn’t mention a lot about them. He says that there are three effects of them on the body, and he wants me to mention them. I remember that they increase ICP, which was correct. He asks me how they do that, and I guess that they vasodilate cerebral arteries, which was correct.
He then says “if they vasodilate the cerebral arteries, what do you think happens with the other arteries in the body?” I guess that they vasodilate as well, potentially causing hypotension, to which he agrees. I say that they have a depressant effect on the heart, to which he agrees and then asks which of them have the least cardiodepressive effect. I had noe idea, so I guess one of them (don’t remember which one), but it was the wrong one. I don’t remember which is the right one.
He asks about the last effect. I don’t know, but he tries to help me by saying that it affects the respiratory system. I remember that some of them cause airway irritation, so that they can’t be used for induction of anaesthesia. He agrees, but that wasn’t what he was looking for. He asks me which of them that can be used for induction. I guess one of them, but it was wrong again. Don’t remember what I guessed or what was correct.
He’s still waiting for the third effect of these drugs. He tries to help me by saying that it’s a very useful effect in the ICU. I had a small hunch that it was bronchodilation, so I guessed it, and it was correct.
He asks me about which patients it’s preferred to use inhalational anaesthetics for induction rather than IV. I remember from the paediatric anaesthesia topic that it’s better for young children, which is what I tell him and he’s very happy. That was the end, and was very satisfied and gave me a nice 5.
Final thoughts
It was a very different experience from what I expected. I expected a short exam with no prep, not this. But he was very enthusiastic when I gave right answers, and he didn’t seem to mind wrong answers too much. He gave helpful hints and was patient, but perhaps a bit intense. I was kinda lucky because 1,5 of my topics was mostly pharma and the other half was mostly psych.
My next exam is neuro on Friday.
Words cannot express my feelings, nor my thanks for all your help. I sincerely I appreciate your generosity. 🌷🌷
You’re very welcome <3
Hello , Congratulations 🎊 ,
Firstly , thank you so much for writing those notes , you are a real life saver!!!!
Do we need to know more than what you’ve written or you really believe those are enough?
Thanks in advance ❤️❤️❤️
Thank you and thank you!
People ask me whether my notes are “enough” constantly, as if I know exactly what examiners need us to know. I don’t, and the only way to know whether they’re “enough” is if people try and use them and see. So ask around if people have used them with success. I know at least a few who have.
For future reference:
MAC is inversely proportional to potency which is why it’s not a measure of it.
The more potent the drug is the lower the minimal alveolar concentration is needed to reach GA.
That’s true, but I also feel like that’s nitpicking. Many sources refer to MAC as a “measure” of potency, even though the relationship is inversely proportional.
Do they use old topic list ?
Because in new list, the topic should be pharmacology of inhalational and IV anesthetics ?
Yeah apparently that was a mix-up at the department. They should use the new topic list now. But they said that they decided to keep the inhalational and IV anaesthetics in separate topics anyway.
Gyn notes plz…
Don’t “gyn notes plz…” me plz… That’s disrespectful
Would drag my balls through broken glass for gyn notes from you. If you want more respect I have a lot more in store <3 <3 <3
<3 please don't.
I plan to write gyn notes before my gyn exam on Thursday.
Words are futile devices.
You’re the true MVP.
LMAOOOOOO 🤣🤣🤣🤣
Thank you for your note and congrats 😀
How many days do u think we need for it ?
Couple of days maybe?
Do you have any suggestions for those of us who get a migraine just looking at the notes that are available? pls help
Triptans and other analgesics 🙂
I made notes, I’ll upload them. Maybe they’ll ease your migraine
Holy. Mother. Of. Christ. 40 pages.
How does one reward such chivalry? 😭
If you appreciate it, you can pay it forward by doing something nice for someone else 🙂