Table of Contents
Page created on March 2, 2019. Last updated on December 18, 2024 at 16:57
Introduction
The liver and lungs share the unfortunate throne of being those organs that are most frequently metastasized into. The most common hepatic neoplasms are neoplastic carcinomas from the colon, lung or breast.
The liver obviously also has primary tumors.
Tumor-like lesions of the liver
Liver cyst
Simple liver cysts may be single or multiple. Patients are almost always asymptomatic, and no specific management is required unless they cause symptoms. It’s easy to distinguish liver cysts from solid lesions on imaging.
Polycystic liver disease
Polycystic liver disease is a condition where many cysts form in the liver, eventually replacing a critical mass of the functional liver, causing liver failure. Hepatomegaly may cause abdominal pain and possibly abdominal distension. Polycystic liver disease may occur alone or as a symptom of polycystic kidney disease.
Focal nodular hyperplasia
Focal nodular hyperplasia (FNH) is a benign lesion consisting of hyperplastic hepatocytes nodules with a characteristic central stellate scar. It is localized and well-demarcated. It’s not a true neoplasm but instead a hyperplastic response to a vascular malformation or portal duct injury.
FNH is the second most common benign liver lesion. It occurs most commonly in middle-aged females. Contraceptives may increase the risk. These lesions are mostly asymptomatic and have no malignant potential and is therefore not usually removed.
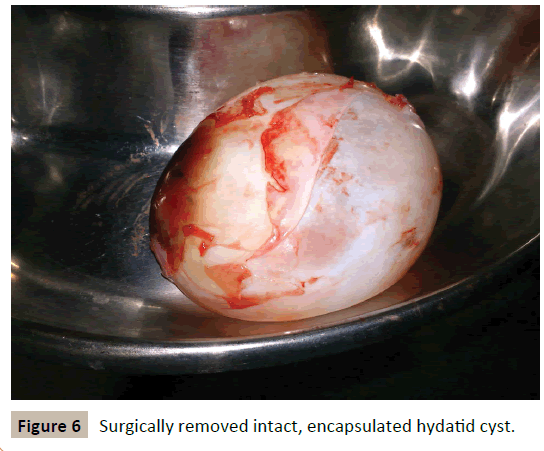
Echinococcus cyst
Echinococcus cysts, also called hydatid cysts, is a consequence of consuming something contaminated by echinococcal tapeworm’s eggs. An example of contamination is drinking water which is infested by dog faeces, or not washing your hands after petting a dog or cat and then touching food. When the eggs are ingested, they hatch in the intestines and the adult tapeworms penetrate the intestinal wall. This gives them the ability to travel with the blood stream or the lymphatic circulation, and they often end up in the liver where they die and form a hydatid cyst. This cyst can grow and compress the structures in the liver and around, destroying the liver parenchyma in the worst case.
The incubation time is long (up to 50 years!), and the cyst shows usually no symptoms. However, the patients may experience pain in the upper right quadrant and hepatomegaly. Rupture of these cysts can cause anaphylaxis and death, so surgery is needed to remove them as soon as possible.
These cysts may look solid on imaging and can therefore be mistaken for a tumor.
These cysts are often solitary, but they can be multiple. This occurs if the parasites can spread throughout the biliary tree before dying.
Liver abscesses
Liver abscesses in Western countries are caused by bacteria, so-called pyogenic liver abscess. In developing countries, liver abscesses are mostly caused by parasites. Liver abscesses mostly affect the right lobe of the liver.
The bacteria can reach the liver by ascending infection in the biliary tract, through vascular seeding from the GI-tract, direct invasion into the liver from a nearby source or by a penetrating injury. The infection is often polymicrobial.
The most common sources of bacterial liver abscesses are:
- Ascending infections from the biliary tract (ascending cholangitis) – most common
- Spreading of bacteria from the GI tract via the portal vein
- Systemic bacteraemia (sepsis)
Bacterial hepatic abscesses can occur alone or as multiple lesions, and their sizes can range from millimetres to many centimetres. The morphology is as for any pyogenic abscess: liquefactive necrosis with neutrophil infiltration.
Antibiotics and drainage are needed. Untreated liver abscesses have a high mortality rate!

A gigantic liver abscess for you to look at
Benign liver tumors
These benign tumors must be differentiated from a carcinoma on imaging or with biopsy.
Hepatic adenoma
Hepatic (or hepatocellular) adenoma is a benign tumor of hepatocytes. It’s rare. It is associated with contraceptive use and is therefore most common in females.
Hepatic adenomas are problematic as they have the possibility to rupture or haemorrhage, which may be life-threatening. They may also undergo malignant transformation into hepatocellular carcinoma. For these reasons, they should be surgically removed and contraception should be stopped.
Hepatic haemangioma
Hepatic haemangioma is a benign vascular lesion of the liver, and the most common liver tumour. It is associated with contraceptive use and is therefore most common in females. The peak incidence is in the 30 – 50s. They’re mostly asymptomatic and have no malignant potential and is therefore not usually removed.
It’s a type of cavernous angioma. These haemangiomas are composed of many endothelium-lined vascular spaces separated by fibrous septa.
Bile duct adenoma
Bile duct adenoma is a rare benign condition of the bile ducts that is often found incidentally. It can easily be confused with a malignant tumor and can therefore interfere with differential diagnosis.
Hepatocellular carcinoma
Introduction and epidemiology
Hepatocellular carcinoma (HCC) is the most common primary malignant tumor of the liver. It’s mostly a disease of older men. In almost all cases it develops in an already cirrhotic liver, so the risk factors for HCC are the same as those for cirrhosis.
The incidence of HCC is increasing.
Etiology
Common causes:
- Chronic HBV or HCV infection
- Non-alcoholic fatty liver disease
- Alcoholic liver disease
- Aflatoxin
Rare causes:
- Hepatotoxic drugs like paracetamol
- Haemochromatosis
- Autoimmune hepatitis
- Alpha-1-antitrypsin deficiency
- Wilsons disease
- Hepatic adenoma
Aflatoxin is a toxin produced by aspergillus fungi that can contaminate food. It can cause HCC without cirrhosis, and is mostly present in developing countries.
Pathology
HCC develops from a dysplastic nodule in a cirrhotic liver. This nodule is a precancerous lesion that can be visualized on ultrasound.
Hepatitis B may incorporate the HBsAg into the host genome. Hepatitis C has no such capacity. Both viruses increase cancer risk due to the chronic inflammation and high cell turnover they cause.
Aflatoxin causes a very characteristic mutation in the p53 gene called a signature mutation. If this mutation is present in an HCC it’s certain that the etiology was aflatoxin. Aflatoxin is a common cause of HCC in the developing world but it’s a rare cause in the Western world.
A special form of HCC called fibrolamellar HCC is very rare. Only 200 new cases are diagnosed every year. This type of HCC develops in young adults without cirrhosis or other risk factors for HCC.
Diagnosis
Patients at high risk for HCC (all with cirrhosis or chronic hep B) are screened with AFP and ultrasound. If these are positive, a CT or MRI is performed. These findings together are usually enough to diagnose HCC, obviating the need for biopsy, which carries a risk for tumour spread.
Prognosis
HCC doesn’t produce significant symptoms until it’s already at an advanced stage. Any symptoms it would produce would be masked by the underlying cirrhosis. It’s also rarely possible to completely excise the tumor. This gives it a poor prognosis.
Other malignant tumors
Intrahepatic cholangiocellular carcinoma accounts for 10% of CCC cases. It’s rare and aggressive. More about this in topic 16.
Hepatoblastoma is a rare childhood tumor that originates in liver precursor tissue, but it’s the most common primary liver tumour in children (0 – 3 years). It usually presents as an abdominal mass.
Hepatic angiosarcoma is very rare and aggressive. It’s notably associated with exposure to certain toxins, vinyl chloride and thorium dioxide. Vinyl chloride was formerly used in the plastic industry. Thorium dioxide was a radiocontrast material formerly used.