Table of Contents
Page created on April 20, 2019. Last updated on December 18, 2024 at 16:57
Introduction
The prostate is divided into several biologically distinct regions:
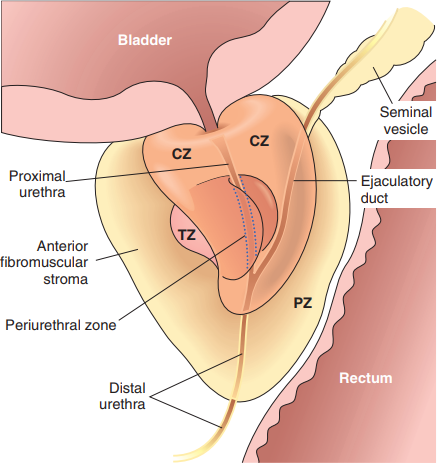
Benign prostate hyperplasia (BPH) occurs in the transitional zone (TZ) and periurethral zone, while most cancers occur in the peripheral zone (PZ).
The prostate is comprised of glands and stroma. The glands are comprised of two cell layers, a flat basal cell layer and a luminal columnar secretory cell layer. The glands are surrounded by a layer of myoepithelial cells. These glands produce the alkaline milky liquid that is added to the semen. The prostatic stroma contains a mixture of smooth muscle and fibrous tissue.
The weight of the prostate depends on the age of the subject, as the prostate continously grows as men age. Normal values for weight range from 15 – 30 g. This study found an average of 38 g even in young organ donors without BPH.
Prostatitis
We distinguish four categories of prostatitis:
- Acute bacterial prostatitis
- Chronic bacterial prostatitis
- Chronic non-bacterial prostatitis
- Granulomatous prostatitis
Acute bacterial prostatitis is most frequently caused by gram-negative bacteria like E. coli. STDs like gonorrhoea and chlamydia may cause prostatitis in sexually active adults.
Symptoms include fever, chills, dysuria and pain in the surrounding area. On digital rectal examination the prostate is swollen, firm and tender.
Diagnosis is based on urine culture. Therapy involves proper antibiotics. It may cause sepsis.
Chronic bacterial prostatitis is caused by the same pathogens as acute bacterial prostatitis. The symptoms, diagnosis and treatment are similar to those of acute bacterial prostatitis.
Chronic non-bacterial prostatitis is also called chronic pelvic pain syndrome and is by far the most common cause of prostatitis. Prostatitis is present on histology but it is uncertain whether the prostatitis is the cause of the symptoms or the result of some other causative factor. Affected patients have chronic pelvic pain and usually other genitourinary symptoms like dysuria. No causative agent is known, but recurring acute prostatitis may be a risk-factor. Diagnosis is based on urinary culture, which shows no culturable pathogens.
Granulomatous prostatitis is a rare condition that is characterised by the presence of epithelioid granulomas. There are many possible causes, including TB, syphilis and other systemic granulomatous diseases. The most frequent cause is a complication of injecting BCG (an attenuated TB strain) into the bladder to treat bladder cancer. This may cause granulomatous prostatitis indistinguishable from tuberculous prostatitis.
Benign prostatic hyperplasia
Benign prostatic hyperplasia (BPH) is a non-neoplastic hyperplasia of the prostatic stroma and glands in the periurethral and transitional zones of the prostate. BPH is not a precancerous lesion and does not increase the risk for prostate cancer. The prostate grows in size to 60 – 100 g. The hyperplasia forms nodules that compress the urethra.
BPH is an age-related change; it occurs in virtually all men as they grow older. It affects 20% of males in their 40s, 70% of males in their 60s and 90% of males in their 80s. Only about 10% of cases of BPH produce clinical symptoms.
Pathogenesis: BPH does not occur in males without androgen activity, so it’s clear that androgens play a role in BPH. The condition is associated with excessive androgen-dependent hyperplasia of stroma and glands. Circulating testosterone is converted into DHT in the prostate by 5α-reductase. DHT is a much more potent growth factor than testosterone. It is hypothesized that the prostate’s sensitivity to DHT increases as the person ages.
Symptoms: Most clinical features of BPH is due to obstruction of the urethra. The symptoms of BPH are together often called lower urinary tract symptoms (LUTS) and involve the following:
- Polyuria and nocturia
- Increased urinary urgency – a strong urge to urinate
- Dysuria – pain upon urination
- Hesitancy – problems initiating the urination
- Excessive dribbling of urine after the urine stream has terminated
- Feeling that voiding is incomplete – the feeling that the bladder isn’t empty after urination
Complications: Residual urine in the bladder increase the risk for urinary tract infection. If the obstruction is severe, hydronephrosis may occur. Due to the obstruction the bladder detrusor muscle must work harder, causing it to hypertrophy and develop characteristic trabeculae on macroscopy.
Therapy: Initial therapy involves blocking the enzyme (5α-reductase) that convert testosterone into DHT with a drug called finasteride. Alpha-1 blockers (like tamsulosin) are used to induce smooth muscle relaxation of the urethra, which widens the urethral lumen and improves symptoms.
Cases that aren’t sufficiently treated by medical therapy must be treated surgically. Transurethral resection of the prostate (TUR-P) involves using a tool that goes through the urethra and scrapes away the transitional and periurethral zones of the prostate, leaving a cavity and the peripheral zone instead. As the peripheral zone is left intact the risk for developing cancer still exists.
Differential diagnosis of digital rectal examination
| Condition | Tenderness | Feel | Surface | Size |
|
Healthy |
Non-tender | Rubbery | Non-nodular | Normal |
|
Acute prostatitis |
Tender |
Hard |
Non-nodular |
Symmetrically enlarged |
|
BPH |
Non-tender |
Rubbery |
Non-nodular |
Symmetrically enlarged |
| Prostate cancer | Non-tender | Hard | Nodular |
Non-symmetrically enlarged |
Hello Nikolas
Chronic non-bacterial prostatitis is the same thing as the chronic pelvic pain syndrome
This is nit-picking but okay. Fixed.
Sorry I didn’t mean that; I appreciate your work, and you’ve saved my a** a lot of times, perfection is impossible, I’ve been commenting couple of times for all good, no name is indicated, if it bothers you I’ll keep them for myself and I’ll stop posting them. Again Thankyou for your amazing work! Stay safe 🤞🏻
Oh, no hard feelings! I appreciate all comments, even if I feel like they are nit-picking. Nothing to apologize for. Keep the comments coming.
Stay safe!
also you wrote that its swollen but in the table, size is normal
thanks.
Fixed and fixed. THanks!
You rock 🤘
hi greek.doctor
in the prostatitis page , yo said that prostate is firm on DRE, but in the table of DDx of DRE, you wrote prostatitis is soft
Normal 30g?! It is 15g, Dr. Kalman would kill you
Come at me bro
Szia, Anonymous
normal is ca. 20g according to Thieme, check page 257 on Thieme atlas for int. organs.
Different sources say different things. The truth is that it varies greatly with age, and so it’s hard to establish a “normal” weight. It doesn’t matter.