Page created on May 12, 2019. Last updated on December 18, 2024 at 16:57
Page created on May 12, 2019. Last updated on December 18, 2024 at 16:57
Vasculitis
Vasculitis is the general term for inflammation of vessel walls, characterised by fibrinoid necrosis and infiltration of the walls by inflammatory cells. The clinical manifestations can vary wildly, but they mostly depend of the area and type of vessel that is affected. Most vasculitides (yes that’s the plural form) affect the smaller vessels, like arterioles, capillaries and venules. The two most common pathomechanisms are immune-mediated inflammation and direct vascular invasion by pathogens. The exact pathomechanism is unknown for most types.
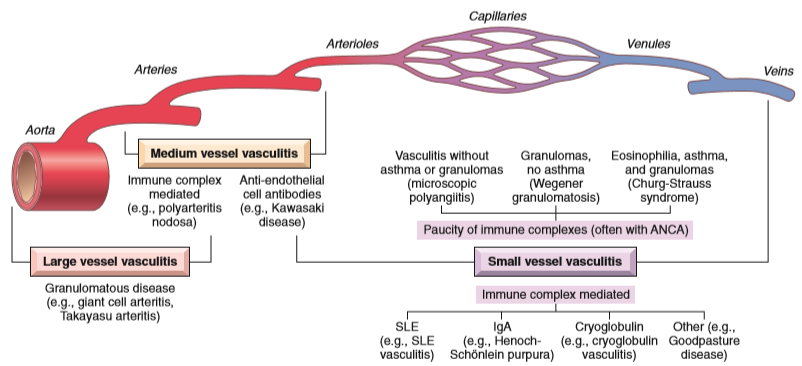
We classify vasculitides based on which type of vessels they target. The important ones are:
- Large vessels
- Giant cell arteritis
- Takayasu arteritis
- Medium vessels
- Polyarteritis nodosa
- Kawasaki disease
- Small vessels
- Microscopic polyangiitis
- Wegener granulomatosis (granulomatosis with polyangiitis)
- Thrombangiitis obliterans
- Any vessel
- Infectious vasculitis
- Vasculitis associated with other diseases
The symptoms and clinical features of each type depends mostly on which type of vessel is targeted, but some non-specific symptoms are common for all types, such as:
- Fever
- Myalgia
- Arthralgia
- Malaise
- Increased erythrocyte sedimentation rate (ESR)
Vasculitides usually cause ischaemia of the tissues that are supplied by the inflamed vessels. Ischaemia can be due to thrombosis on the inflamed endothelium or due to fibrosis occluding the lumen. This is what causes most specific symptoms.
All types except the pathogen-associated ones are treated with corticosteroids. Let’s dive into them.
Large vessel vasculitides
These vasculitides affect the aorta and its major branches.
Giant cell arteritis commonly affects the elderly (>50 years), and most commonly affects branches of the carotid artery, especially the temporal artery. The affected vessels are thickened, and the lumens are narrowed. Microscopically we can see granulomatous inflammation with giant cells. Characteristic for the disease however is how only certain parts of the affected artery are inflamed (skip lesions), so biopsy samples could miss the affected area, resulting in a false negative diagnosis.
The symptoms depend on which artery is affected. Ophthalmic involvement can cause blindness, temporal involvement can cause headache, arteries supplying the face can cause claudication while chewing and so on.
Takayasu arteritis is also a granulomatous arteritis very similar to giant cell arteritis except that it mostly affects the aortic arch and its branches. It mostly affects younger people (< 50 years). Because the subclavian arteries can be affected the pulse in the wrists can be very weak or missing. Carotid involvement can cause visual disturbances. Narrowing of the coronary arteries can cause myocardial infarction. Histologically mononuclear (macrophages, lymphocytes) infiltration and giant cells can be seen.
Medium vessel vasculitides
These vasculitides affect muscular arteries that supply organs.
Polyarteritis nodosa is a necrotizing vasculitis that usually affects the renal and visceral vessels. It most commonly occurs in young adults. Histologically can we see transmural fibrinoid necrosis, often with mural thrombosis. The inflammatory infiltrate contains neutrophils, macrophages and eosinophils. Old lesions become fibrous and thickened, small aneurysms form, which is what gives the affected artery the “nodular” appearance, hence the name.
What’s characteristic for this condition is that it usually contains lesions that are in different stages of the disease. Some lesions are very young and necrotic, while some lesions are old and fibrotic.
The symptoms depend on the affected vessel. Renal artery involvement can cause renovascular hypertension, while mesenteric artery involvement can cause abdominal pain and melena. The lung is usually not affected.
Kawasaki disease is unlike the others an acute, self-limiting disease (meaning that it resolves itself) that usually occurs in infancy and childhood. It usually affects the coronaries, which can cause myocardial infarctions in these young children. The histology is similar to in polyarteritis nodosa.
Other clinical symptoms are non-specific and include fever, conjunctival and oral erythema, oedema of the hands and feet, skin rashes and cervical lymph node enlargement.
Small vessel vasculitides
These vasculitides affect arterioles, capillaries and venules.
Many small vessel vasculitides involve a special type of antibodies. These antibodies recognize and bind to proteins that are inside the cytoplasm of neutrophils. The antibodies are therefore called anti-neutrophil cytoplasmic antibodies, or ANCAs. Two types are important, ANCAs that target a protein called proteinase 3 (PR3-ANCAs), and ANCAs that target myeloperoxidase (MPO-ANCAs).
Thrombangiitis obliterans (Buerger disease) is characterized by acute and chronic inflammation of medium and small arteries, especially the tibial and radial arteries. Thrombosis usually occurs, usually with small microabscesses. The inflammation often extends into nearby veins and nerves, which is unique for vasculitides.
Most affected people are smokers. Gangrene and severe pain in the limbs is common.
Wegener granulomatosis (polyangiitis with granulomatosis) is a systemic disease with a necrotizing vasculitis component. It affects the nasopharynx, lungs and kidneys. It has three characteristic findings:
- Granulomas in the lung and/or upper respiratory tract
- Vasculitis, most prominently in the lung and upper respiratory tract
- (Rapidly progressive) glomerulonephritis
The vasculitis is necrotizing and granulomatous. PR3-ANCAs are involved. The mortality rate of untreated persons is very high.
Microscopic polyangiitis is a necrotizing vasculitis that involves arterioles, capillaries and venules. It’s very similar to Wegener, except the nasopharynx isn’t involved and there are no granulomas. Almost any organ can be involved, but it almost always affects the lung and kidney. It’s associated with MPO-ANCAs.
- (Rapidly progressive) glomerulonephritis
- Lung and upper respiratory tract vasculitis
Depending on which vascular bed that is involved can the symptoms vary. Haemoptysis, haematuria, proteinuria and palpable purpuras in the skin are common.
Vascular tumors
Both benign and malignant tumors can occur in vessels. We have (roughly) three types:
- Common and benign
- Cavernous haemangioma
- Capillary haemangioma
- Kasabach-Merit syndrome
- Von Hippel-Lindau disease
- Cavernous lymphangioma
- Locally aggressive, but infrequently metastatic neoplasms
- Kaposi sarcoma
- Haemangioendothelioma
- Rare, highly malignant angiosarcomas
Benign vascular tumors
Haemangiomas are very common benign tumors composed of blood-filled vessels. The most important complication of them is that the large ones can compress nearby structures, and they can rupture and cause bleeding. They often affect the skin and liver. Multiple types exist, including:
- Capillary haemangiomas are the most common type. They occur in the skin, mucous membranes, liver, spleen and kidneys. They form small nodules.
- Cavernous haemangiomas mostly affect the liver. The vessels are dilated, making them look like cavernas.
- Von Hippel-Lindau disease is a genetic disease where cavernous haemangiomas occur in characteristic places of the CNS, like cerebellum, eye and brain stem. They also develop other tumors like pheochromocytoma and renal cell carcinoma.
Mostly locally aggressive vascular malignancies
Epithelioid haemangioendothelioma is a rare vascular tumor that usually occurs in adults. They usually occur alone, and in most cases are associated with large vessels. The tumor cells are epithelioid in shape.
Kaposi sarcoma was described by a Hungarian guy, so of course it’s included. It can occur in healthy people but is by far most common in patients with AIDS. It’s associated with HHV-8 infection. Four types exist:
- Classic Kaposi sarcoma usually affects elderly males
- Endemic Kaposi sarcoma – occurs in African children and has organ manifestations
- Transplantation-associated Kaposi sarcoma
- Kaposi sarcoma in AIDS – occurs in 30% of all AIDS patients.
Kaposi sarcomas appear macroscopically as red, livid patches, plaques and nodules on the lower extremities mostly. For microscopy, see the slide.
Angiosarcoma
Angiosarcomas are malignant tumors of endothelial cells. They’re highly aggressive and commonly occur in the skin or liver. They’re associated with lymphoedema, radiation and certain chemicals.
Hei! Something seems to be missing at the end there, got me curious
fixed in the best way possible