Table of Contents
Page created on May 22, 2019. Last updated on December 18, 2024 at 16:56
Introduction
A heterotopic disorder of the heart means that something other than the sinoatrial node works as the pacemaker.
Active heterotopy means that the heterotopic focus produces stimuli at a higher frequency than the sinus node. The opposite would be passive heterotopy.
The following conditions are active heterotopic abnormalities:
- Extrasystoles/premature beats
- Atrial fibrillation
- Atrial flutter
- Paroxysmal atrial or ventricular tachycardia
The latter three have their own topics, so only extrasystoles will be examined in this topic.
An extrasystole is a beat that comes earlier than expected according to the heart rate. We distinguish two types, one of which has two subtypes:
- Supraventricular extrasystole
- Atrial extrasystole
- Junctional extrasystole
- Ventricular extrasystole
Extrasystoles may occur randomly, or they can occur in patterns. The following patterns are the most frequent:
- Couplet – two extrasystoles in a row
- Triplet – three extrasystoles in a row
- Bigeminy – one extrasystole occurs after every sinus beat
- Trigeminy – one extrasystole occurs after every two sinus beats
Compensatory pause
After an extrasystole the pacemaker cells will be in the refractory state for a short time, meaning that they can’t conduct signals during that time. The compensatory pauses of supraventricular and ventricular extrasystoles are different and can be used to differentiate them.
If a normal atrial beat is followed by an atrial or junctional extrasystole the extrasystole will conduct through the SA node and reset the timing of the node. Because the SA node has been “reset” it will fire again sooner than if it wasn’t reset. The time from the last R wave before the ES and the first R wave after the ES will be less than 2 x RR-intervals. In other words, the first beat after the ES occurs earlier than we would expect according to the heart rate. There was no compensatory pause.
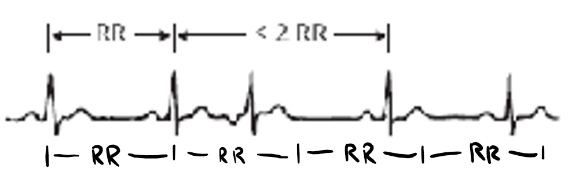
No compensatory pause in supraventricular extrasystoles. As you can see, the first R-wave of after the extrasystole occurs earlier than it would if there was no extrasystole.
If a normal atrial beat is followed by a ventricular extrasystole the extrasystole will not conduct through the AV node and reset the SA node. The SA node will continue at the normal rate, but the ventricular myocardium will be in a refractory state. When the SA node fires the next time, the signal will not be conducted as the ventricles are still in the refractory state. When the SA node fires the next time after that the ventricular myocardium will no longer be in a refractory state, so the signal is conducted normally. The time from the last R wave before the ES and the first R wave after the ES will be equal to 2 x RR-intervals. In other words, the first beat after the ES occurs exactly when we would expect according to the heart rate. There has been a compensatory pause.
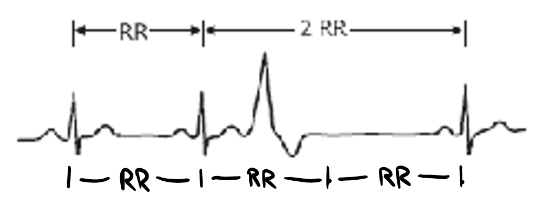
There is a compensatory pause in ventricular extrasystoles. The first R-wave after the extrasystole occurs exactly where it would be if there was no extrasystole.
Supraventricular extrasystoles
Supraventricular extrasystoles (SVES) are called that because they originate supraventricularly. Atrial extrasystoles originate from within the atrial myocardium. Junctional extrasystoles originate from between the atria and ventricles.
SVES don’t significantly impair cardiac output on their own but are dangerous as they might lead to more severe arrhythmias. They may be asymptomatic, but they often cause palpitations.
Etiology:
These beats are often idiopathic and can even occur in healthy hearts. Smoking, alcohol and coffee can trigger these beats in sensitive individuals.
Pathological causes:
- Ischaemic heart disease
- Atrial dilation
- Electrolyte imbalance
Morphology on ECG:
Atrial extrasystole:
- P-wave is abnormal
- Can be positive if heterotopic focus is close to SA node
- Can be negative if heterotopic focus is close to AV node
- PQ-interval is abnormal
- QRS is normal
- No compensatory pause
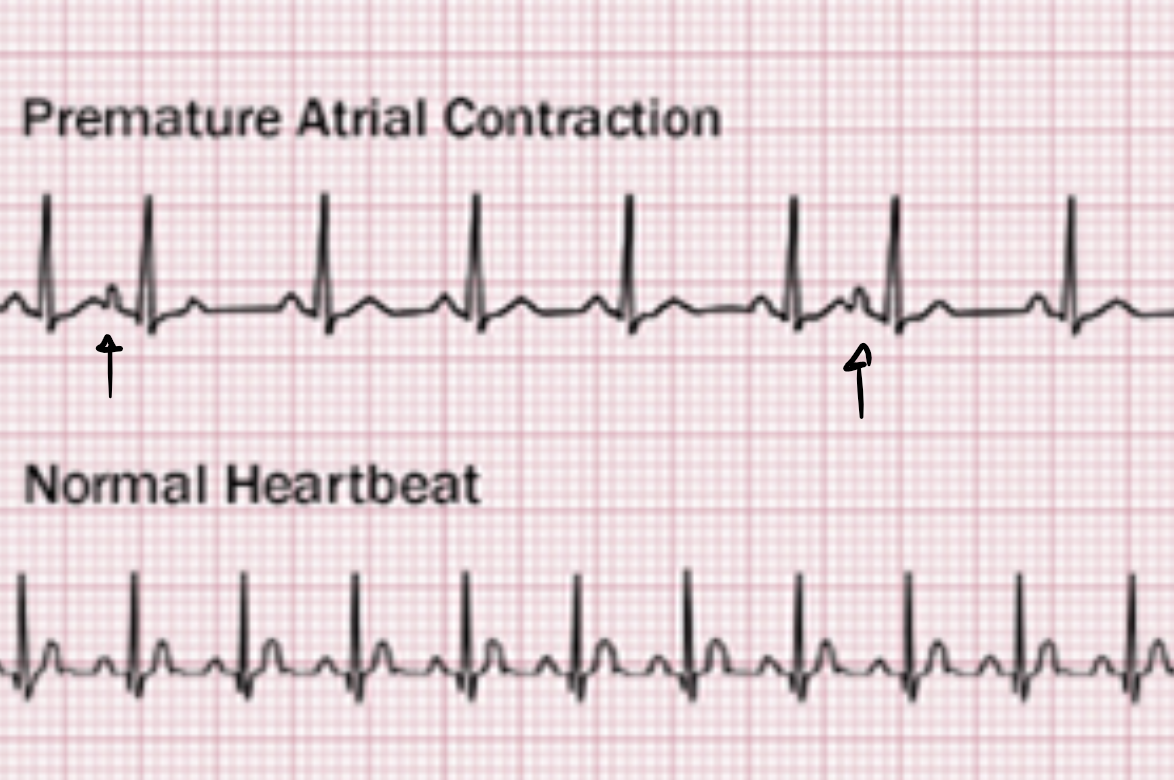
From https://www.webmd.com/heart-disease/atrial-fibrillation/premature-atrial-contractions#1
Junctional extrasystole:
- Negative P-wave
- PQ-interval is abnormal
- QRS is normal
- No compensatory pause
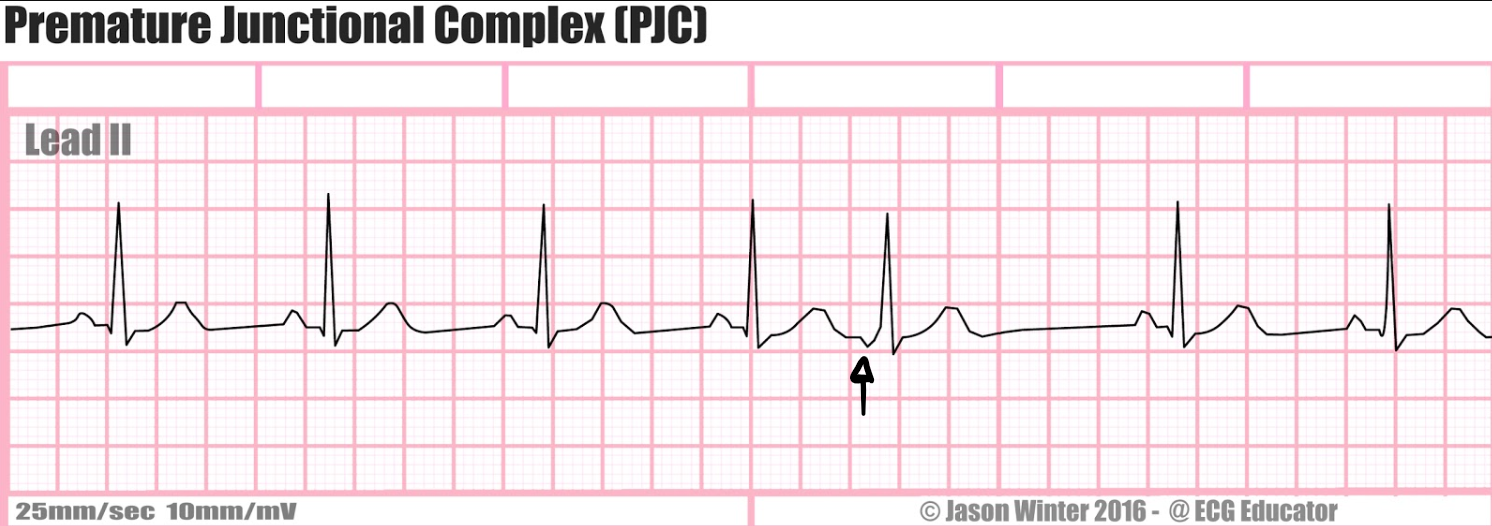
From https://ecg-educator.blogspot.com/2016/11/premature-junctional-complex-pjc.html
Treatment:
Treatment is not needed in asymptomatic individuals. If there are any underlying conditions they should be treated.
Beta blockers or ablation can be performed in symptomatic individuals.
Ventricular extrasystoles
Ventricular extrasystoles (VES) originate from a heterotopic focus in the ventricular myocardium. It is a relatively normal occurrence and occurs in up to 80% of healthy people during a 24-hour ECG monitoring.
Palpitations and the sensation of a skipped beat are common symptoms. Ventricular extrasystoles can alter the cardiac output, especially if many occur in a short amount of time (bigeminy or many couplets).
Etiology:
Like SVES these beats are often idiopathic and are frequently seen in people with no heart disease. Some people are sensitive to alcohol and caffeine and may develop VES after ingesting these.
Pathological causes:
- Ischaemic heart disease
- Digitalis toxicity
- Myocarditis
- Electrolyte imbalance
Morphology on ECG:
Ventricular extrasystoles can be monomorphic or polymorphic. Monomorphic VES’ originate from the same heterotopic focus and therefore have similar morphology. Polymorphic VES’ originate from multiple heterotopic foci and will therefore have different morphology.
The following characteristics can be seen on ECG:
- P-wave does not precede the QRS complex
- QRS complex is wide
- A compensatory pause follows the extrasystole
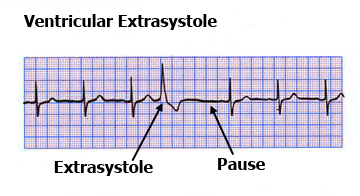
From http://www.doctortipster.com/3744-ventricular-extrasystoles-causes-diagnosis-and-treatment.html
Complications:
If a VES occurs so that the R-wave coincides with the peak of a T-wave of the preceding beat, ventricular fibrillation or flutter can be the result. This is called the “R on T phenomenon”. R on T phenomenon does not always lead to ventricular arrhythmias; they usually only do so when there are other contributing factors present, like ischaemia.
Treatment:
Treatment is not needed in asymptomatic individuals. Any underlying condition should be treated.
If VES’ occur frequently or cause symptoms they can be treated with ablation.
Szia, Nik
This statement is wrong: “The coupling time is the time between the peak of the R-wave in the extrasystole and the peak of the R-wave in the following beat.”
Coupling time is the time btw. the last normal R-wave and the R-wave in the extra systole.
Correct. Removed as it wasn’t important for the explanation anyway.