Table of Contents
Page created on November 6, 2019. Last updated on December 18, 2024 at 16:55
The circulatory system
The circulatory system is divided into many different parts. The systemic circulation is the one which supplies all tissues of the body with oxygenated blood and nutrients. The vast majority of blood is in the systemic circulation. The systemic circulation begins at the aorta and ends at the superior and inferior vena cavae. It has an arterial and a venous side, where the arterial side contains oxygen-and-nutrient-rich blood and the venous side contains oxygen-and-nutrient poor blood.
The pulmonary circulation is much smaller. Like the systemic circulation it has an arterial and a venous side, but unlike the systemic circulation the arterial blood in the pulmonary circulation is oxygen-poor, while the venous blood is oxygen rich. The blood is also nutrient-poor at both ends. The function of the pulmonary circulation is not to provide nutrients and oxygen to the lungs but rather to saturate deoxygenated blood with oxygen.
The systemic circulation is divided into multiple parts:
- The arteries
- The arterioles
- The capillaries
- The venules
- The veins
Arteries:
The function of arteries is to transport blood under high pressure to the tissues. To do this the arteries have strong vessel walls, and blood flows at high velocity in the arteries.
Arterioles:
The arterioles are the last small branches of the arterial system. They act as the gates between the arterial and capillary system, intelligently selecting which capillaries should receive the most blood flow.
Arterioles have strong muscular walls which allows them to change the size of their lumen considerably. They can constrict so much that the lumen is completely closed, or they can dilate so that the lumen becomes very large.
The arterioles are the vessels which account for most of the total peripheral resistance (TPR).
Capillaries:
It’s at the level of the capillaries that fluid, nutrients, electrolytes, hormones and other substances are exchanged between the blood and the interstitial fluid. To allow this, the capillary walls are thin and have many pores which are permeable to water and other small molecules.
More about capillary circulation in topic 35.
Venules:
The venules collect blood from the capillaries and gradually combine to form larger veins.
Veins:
The veins transport blood back to the heart. The pressure inside the veins is very low, so the walls of the veins are thin. Even so, they are muscular enough to contract or expand. This allows them to act as a controllable reservoir for extra blood, a blood “storage site”. Indeed, the veins contain most of the blood in the body.
The vein reservoir can be emptied if the veins vasoconstrict. This increases the venous return which will, thanks to the Frank-Starling mechanism, increase the cardiac output, thereby increasing the amount of blood in the arterial circulation.
Cross-sections and velocities of the different parts of the circulatory system:
|
Vessel |
Cross-sectional area (cm2) | Velocity of blood flow (cm/s) |
|
Aorta |
2.5 | 33 |
|
Small arteries |
20 | 4,1 |
|
Arterioles |
40 | 2,07 |
| Capillaries | 2500 |
0,03 |
| Venules | 250 |
0,33 |
| Small veins | 80 |
1,03 |
| Venae cavae | 8 |
10 |
Note how slow blood flows in the capillaries compared to the arteries. The capillaries are typically between 0,3 and 1 millimetre in length, so blood only stays in the capillary for 1 to 3 seconds. During this short time all nutrients and stuff in the blood must diffuse across the capillary wall.
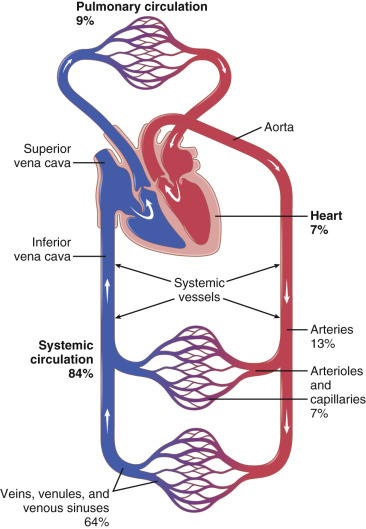
The organization of the circulatory system. The percentages show how much blood is present at the different parts.
Blood pressure
The blood pressure refers to the pressure the circulating blood exerts on the walls of the blood vessels. It is a form of hydrostatic pressure. The blood pressure differs considerably in the different parts of the circulation. As blood flows from the aorta through the systemic circulation the pressure falls progressively to around 0 mmHg by the time it reaches the right atrium.
When we talk about “blood pressure” we usually refer to the arterial blood pressure.
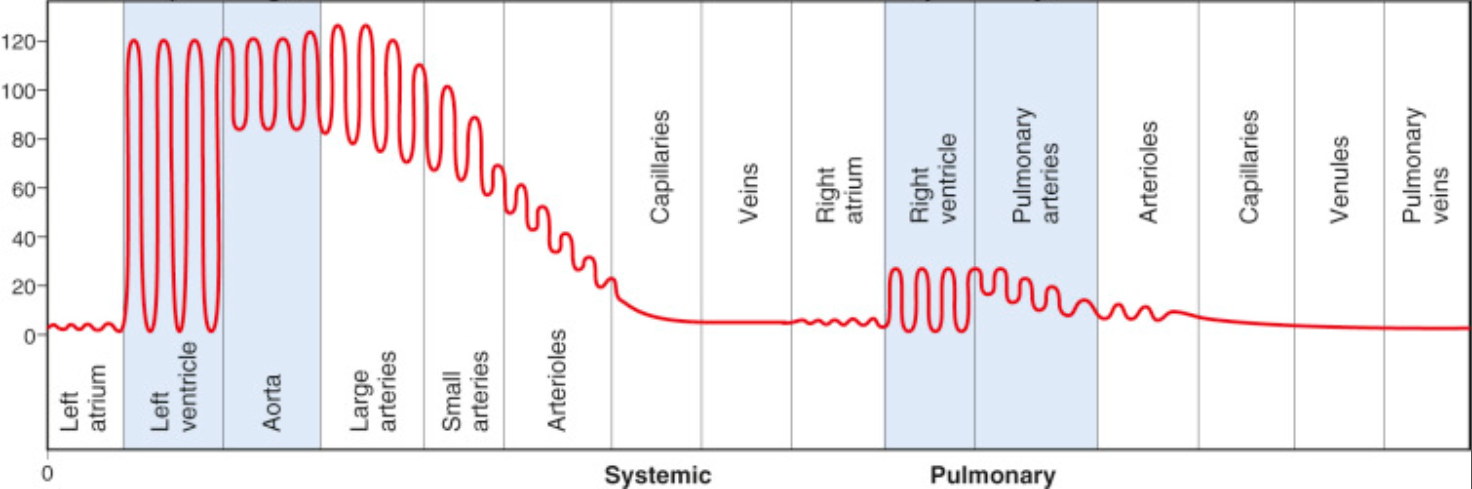
Blood pressure in the different parts of the circulatory system.
The blood pressure in the arteries increases and decreases with each cardiac cycle. When the heart contracts and ejects blood during systole the pressure inside the arterial circulation increases for a short while. During diastole the blood pressure is around 80 mmHg. When systole comes, the blood pressure increases by about 40 mmHg, to about 120 mmHg. The same pattern does not occur in the capillaries and veins, as seen on the figure above.
The blood pressure during systole is called the systolic blood pressure (SBP) while the blood pressure during diastole is called the diastolic blood pressure (DBP). Both pressures are important, so when measuring the blood pressure of a person we always measure both values. We say that the normal blood pressure is around 120/80 mmHg, pronounced “120 over 80 millimetres of mercury” or simply “120 over 80”. The systolic blood pressure is always higher than the diastolic.
The difference between the systolic and diastolic blood pressure is called the pulse pressure. Pulse pressure = systolic blood pressure – diastolic blood pressure
We can calculate the mean arterial pressure (MAP), which is the average blood pressure in the arteries during a single cardiac cycle. The following formulas relate the MAP to the systolic and diastolic blood pressure:

The following formula is also valid:
Determinants of blood pressure:
There are multiple factors which influence the blood pressure:
- Cardiac output
- Heart rate
- Stroke volume
- Blood volume
- Total peripheral resistance
- Viscosity of the blood
- The elasticity of vessel walls
The blood pressure increases if any of the first 4 factors increase. If the blood vessels walls become less elastic (i.e., more rigid), the blood pressure also increases. The only exception is elasticity of vessel walls. Decreased elasticity means stiffer vessel walls and therefore increased blood pressure.
Normal values of blood pressure at different points:
| Systolic pressure (mmHg) | Diastolic pressure (mmHg) | |
|
Aorta (arterial circulation) |
120 – 140 |
60 – 80 |
| Pulmonary trunk (pulmonary circulation) | 20 – 24 |
9 – 15 |
Fluctuations of blood pressure:
The blood pressure varies throughout the day and with physical activity or emotional stress.
- During sleep – both SBP and DBP decrease
- During emotional stress – SBP increases but not the DBP
- During physical activity – SBP increases but not the DBP
The diastolic blood pressure is mostly constant during the time spent awake, although it does decrease while sleeping. The systolic blood pressure on the other hand changes more often, especially during exercise.
Vascular compliance
Compliance is an important concept in physiology. It described how much a hollow organ, such as a blood vessel, can distend and increase its volume. If an organ can distend easily it has high compliance. If an organ cannot distend it has poor compliance. When talking about blood vessels we can say that a vessel has high compliance if it can increase the diameter of its lumen a lot when needed.
Veins have much higher compliance than arteries. This is what allows the veins to act as a “reservoir” for blood, as the veins can distend easily and therefore hold more blood.
Measuring the blood pressure
Blood pressure is routinely measured nowadays by automatic machines, but it can also be measured manually. The machines measure the blood pressure by the same principles as the manual way. This method is often called Riva-Rocci in Hungary, or simply RR.
The Riva-Rocci method requires a stethoscope and a sphygmomanometer, also known as a blood pressure meter. The sphygmomanometer consists of an inflatable cuff which goes around the upper arm, a measuring unit and a pump to inflate the cuff. The measuring unit is often a pressure gauge.
When inflating the cuff, it will squeeze the arm by applying pressure on it. The exact amount of pressure exerted by the cuff on the arm can be read from the measuring unit. The more the cuff is inflated, the more pressure it will exert on the arm. The pressure it exerts on the arm will work to compress the arteries in the arm.
When the cuff is inflated so much that the pressure it exerts on the arm is higher than the diastolic blood pressure of the person (but less than the systolic blood pressure), the arteries in the arm will be closed during diastole. With every systole the arteries will open, because the pressure of the blood on the arterial wall is higher than the pressure of the cuff on the arm, so the blood pressure will keep the arteries open.
When the cuff is inflated so much that the pressure it exerts on the arm is higher than the systolic blood pressure the arteries will be closed until the cuff is deflated. The pressure of the cuff is so large that even the pressure inside the arteries cannot keep them open.
When the cuff pressure is between the systolic and diastolic blood pressure the arteries will open and close with each cardiac cycle. This produces turbulent blood flow, which produces sounds which can be heard with the stethoscope. These sounds are called Korotkoff sounds. These sounds are heard once every heartbeat.
Procedure:
- The cuff is inflated to around 180 mmHg. Place the stethoscope on the cubital region.
- Slowly deflate the cuff.
- As the cuff is slowly deflated a Korotkoff sound can be heard. The cuff pressure when this Korotkoff sound can be heard is equal to the systolic blood pressure of the patient.
- Continue slowly deflating the cuff. The Korotkoff sound can still be heard.
- As the cuff is continuously slowly deflated the Korotkoff sounds will eventually disappear. The cuff pressure when the sounds disappear is equal to the diastolic blood pressure of the patient.
- Deflate the cuff fully.
Example:
- I inflate the cuff to 180 mmHg. I place the stethoscope on the cubital region.
- I slowly deflate the cuff.
- Eventually, I start to hear sounds in the stethoscope. I stop deflating the cuff and note the cuff pressure at this point, which is 140 mmHg.
- I continue to deflate the cuff slowly. The sounds are still present.
- Eventually, the sounds disappear completely. I stop deflating the cuff and note the cuff pressure at this point, which is 90 mmHg.
- I fully deflate the cuff.
The blood pressure of this patient is 140/90 mmHg.
Korotkoff sounds:
There are five Korotkoff sounds but only three of them are important:
|
Korotkoff sound |
Description | Blood pressure equivalent |
|
1st Korotkoff sound |
The first sound which is during cuff deflation | Systolic blood pressure |
| 4th Korotkoff sound | When the sounds become muffled and soft |
Slightly above the diastolic blood pressure |
| 5th Korotkoff sound | When the sounds disappear completely |
Diastolic blood pressure |
Regulation of arterial blood pressure
The body has many mechanisms to regulate the blood pressure, both upwards and downwards. The major mechanisms are:
- The baroreceptor reflex
- Topic 48
- The renin-angiotensin aldosterone system (RAAS)
- Topic 75
- Vasoconstrictor molecules
- Vasopressin/antidiuretic hormone
- Angiotensin II
- Endothelin
- Vasodilator molecules
- Atrial natriuretic peptide (ANP)
- Prostacyclin
- Nitric oxide (NO)
More about the specific mechanisms in their respective topics.
Thank you so much for taking out your time to compile these notes for us! They’ve been so helpful.
Thank you for your comment!