Table of Contents
Page created on December 20, 2021. Last updated on December 18, 2024 at 16:57
Cardiotocography
Definition
The non-stress test (NST) and contraction stress test (CST) are two tests which use cardiotocography (CTG) to measure how the foetal heart rate (FHR) changes in response to foetal movements and oxytocin-induced uterine contractions, respectively.
The cardiotocograph is a diagnostic tool which records both the foetal heart rate and the uterine contractions with the help of two electrodes placed on the mother’s abdomen. It gives information of the foetal wellbeing. One electrode measures the FHR, the other the uterine contractions. The mother is usually given a button to press when she feels foetal movements, which are then recorded by the CTG. The CTG then records the foetal heart rate, uterine contractions, and registered foetal movements over time on a strip, similar to an ECG. The strip may be shown on a screen or printed.
If the water has broken (physiologically or due to amniotomy), the foetal heart rate electrode can be placed on the foetal head through the vagina. This is used for intrapartum monitoring.
Indications
Cardiotocography may be used for multiple purposes:
- Non-stress test
- Routine screening
- In case of a complication during pregnancy or delivery – to ensure the wellbeing of the foetus
- Contraction stress test
- During labour (intrapartum monitoring) – in case of high-risk births
Physiology and rationale
Like for a developed heart, the foetal heart rate is continuously regulated up and down by various factors. CTG allows us to see the foetal heart rate, and how it changes over time in response to foetal movements and uterine contractions.
On the CTG, there will be a baseline foetal heart rate. Physiologically, the heart rate should show considerable beat-to-beat variability from the baseline, i.e. the heart rate should oscillate between higher and lower frequencies with each cardiac cycle. This is called short-term variability and is much more pronounced in foetal hearts than developed hearts. This makes the healthy FHR trace more of a jagged line than a straight line, as it would be in adults.
Long-term variability refers to changes in the FHR which last for multiple cardiac cycles. This includes accelerations and decelerations, and occurs in relation to uterine contractions or foetal movement.
Physiological findings
The foetal baseline heart rate should not be too low or too high. The normal range is 110 – 160 bpm.
A normal ECG will also show accelerations, which are short periods where the foetal heart rate is increased compared to the baseline, after which it returns to the baseline. Accelerations are physiological responses to physical activity, such as the foetus moving, as well as uterine contraction. According to the definition, it only counts as an acceleration if it lasts more than 15 seconds but less than 10 minutes, and if the increase in heart rate is > 15 bpm compared to baseline.
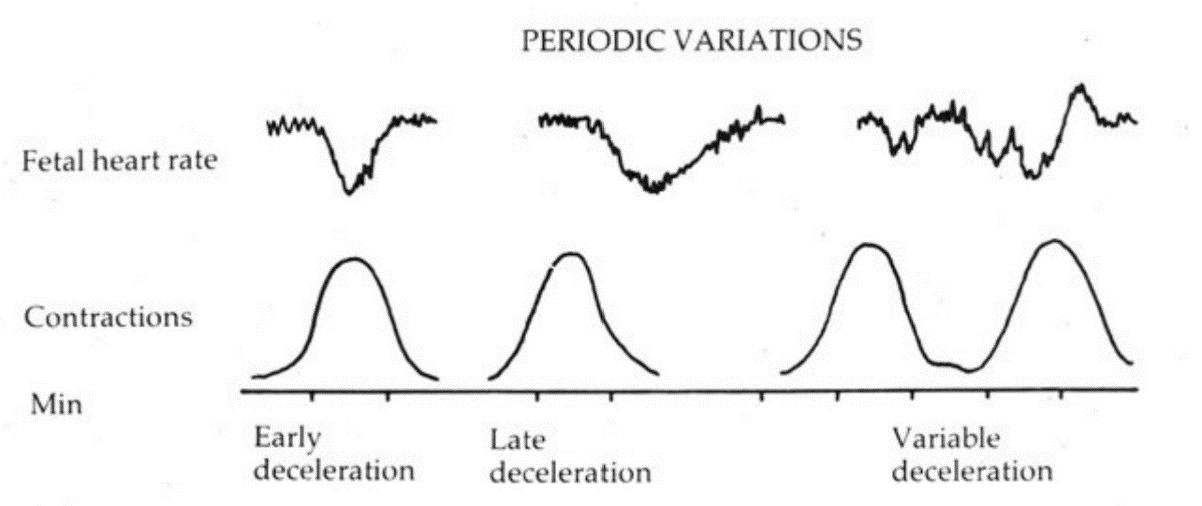
Early decelerations may also be present and are physiological. A deceleration is a short period where the foetal heart rate is decreased compared to the baseline. “Early” refers to how these decelerations occur early after a uterine contraction (more specifically, the deceleration begins when the contraction begins and it reaches its lowest point when the contraction reaches its maximum). This occurs due to the contraction compressing the foetal head, which triggers a vagal response.
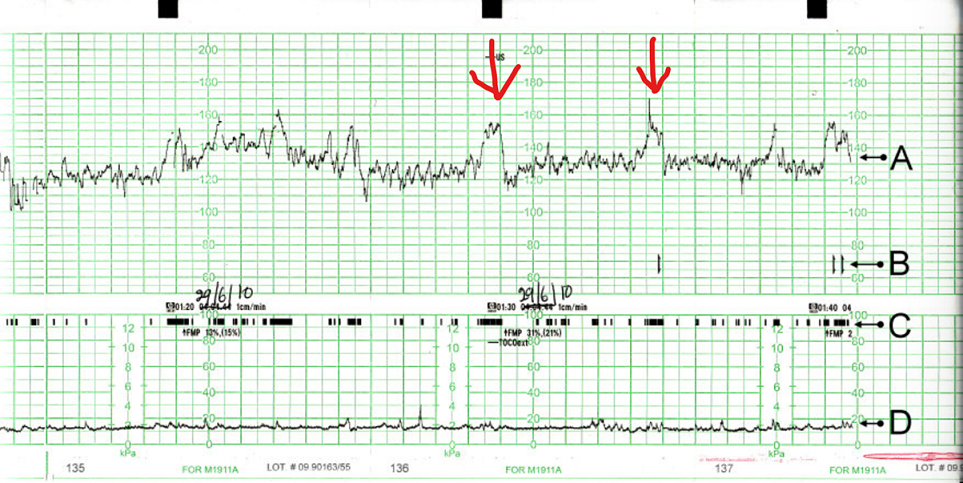
A normal CTG reading. A shows the foetal heart rate reading. B shows the indications when the mother felt movements. C shows the foetal movement, as detected by the machine. D shows the reading of uterine contractions. The red arrows show two accelerations (but there are more accelerations present). From https://commons.wikimedia.org/wiki/File:CTG_Output.jpg
Pathological findings
- Abnormalities of baseline FHR
- Foetal tachycardia (> 160 bpm)
- Foetal bradycardia (< 110 bpm)
- Abnormalities of short-term variability
- Decreased variability (short-term variability of < 5 bpm)
- Absent variability (no variability, straight line)
- Increased variability (short-term variability of > 25 bpm)
- Abnormalities of long-term variability
- Late deceleration (decelerations which occur late)
- (Late refers to that the deceleration doesn’t begin until the contraction has already reached its maximum)
- Variable deceleration (deceleration which occur at varying times compared to the contraction)
- Sinusoidal heart rate (FHR changes up and down in a way that makes a sinusoidal waveform)
- Late deceleration (decelerations which occur late)
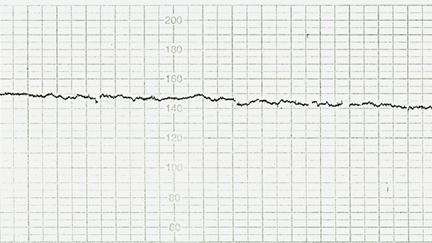
A CTG with absent FHR variability, both short-term and long-term. From http://eknygos.lsmuni.lt/akuserijaen/Obstetrics/4%20CTG%20engl.html
Interpretation
| CTG abnormality | Typical cause |
| Tachycardia | Maternal fever or as a side effect of drugs |
| Bradycardia | Hypoxia or defects in the heart or CNS |
| Decreased/absent variability | Placental insufficiency -> hypoxia, acidosis |
| Late deceleration | Placental insufficiency -> hypoxia, acidosis |
| Variable deceleration | Umbilical cord compression |
| Sinusoidal heart rate | Foetal anaemia |
Presence of any of these findings on CTG is worrying for the foetal status and should prompt intrauterine resuscitation or immediate delivery. If the variability is absent, the CTG is preterminal, meaning that the foetus is in a preterminal state.
ST events
Modern CTG machines can also analyse the ST-segment of the foetal ECG. This is called STAN (ST ANalysis). STAN can give additional information regarding the foetal status. More specifically, the ST-segment gives information on the oxygenation of the foetal heart, which, when interpreted together with the CTG, increases the specificity.
STAN requires the electrode for the foetal heart rate to be placed on the foetal head (i.e., the membranes must have ruptured), so it can only be used during labour and not during NST or CST.
During STAN, the machine will continuously analyse the foetal ST segment for elevation or biphasic ST-segment and can give a notification if abnormal.
Nonstress test
As already described, the nonstress test (NST) is a test of foetal condition which uses cardiotocography to describe how the foetal heart rate changes in response to foetal movements. The test must last for 20 minutes to be conclusive.
NST is simply what we call antenatal CTG investigation without oxytocin administration. In some countries (like Norway), the term NST is not used, and the investigation is simply called “antenatal CTG” instead.
The main use of NST is to rule out foetal abnormality in high-risk pregnancies in an outpatient setting. NST should not be used to screen healthy women with seemingly healthy pregnancies (although this is still performed sometimes). To avoid unnecessary procedures and interventions, low-risk pregnancies should not routinely undergo NST.
Rather than talking about physiological or normal NST, we say it’s “reactive”. An NST is reactive if 2 or more accelerations are seen during the 20 minutes. A reactive test means that there is a low risk for foetal acidosis, and it can be reasonably concluded that the foetus is oxygenated normally.
The test is nonreactive if < 2 accelerations occur. This may be a sign of abnormality and should prompt further investigation. A nonreactive test means that there is an increased risk for abnormality in the foetus, but it can also be due to the foetus sleeping. In case of a nonreactive test, vibroacoustic stimulation should be performed to rule out sleeping as a cause. This involves a device which is placed on the maternal abdomen and produces vibrations and sound.
Of course, if any of the pathological findings detailed earlier are present, the test is abnormal and immediate measures must be taken. However, these findings are more frequently seen during birth or maternal illness, and are rarely seen in the setting in which NST is performed.
Contraction stress test
Also called oxytocin challenge test (OCT), the contraction stress test (CST) is similar to the NST but involves giving IV oxytocin to stimulate uterine contractions. This test is often performed if the NST is non-reactive.
A CST is normal (negative) if early decelerations occur, and abnormal (positive) if late or variable decelerations occur. An abnormal CST may be an indication for further investigations (biophysical profile, etc.) or even delivery.
Despite NST and CST being widely used, there is no good evidence that they actually improves any endpoints of value (perinatal mortality, number of C-sections, etc.)