Table of Contents
Page created on February 25, 2019. Last updated on December 18, 2024 at 16:57
Introduction
Hypertension is the most common cardiovascular disease. Its diagnosis should be based on repeated blood pressure measurements under calm conditions.
- Mild hypertension – 140/90 to 159/99 mmHg
- Moderate hypertension – 160/100 to 179/109 mmHg
- Severe hypertension – >180/110 mmHg
Hypertension may be secondary to a condition like Cushing’s or pheochromocytoma, but it’s most commonly primary.
The blood pressure depends on the cardiac output and the total peripheral resistance (TPR). This gives multiple target areas to influence the blood pressure:
- The arterioles, which determine the TPR
- The heart, which determines the cardiac output
- The kidney, which determines the vascular volume and TPR
The following drug types are the most important in treating hypertension:
- ACE inhibitors
- Angiotensin receptor blockers
- Thiazide and thiazide-like diuretics
- Calcium channel blockers
- Beta blockers
The others are less commonly used.
Diuretics
The role of Na+ in hypertension is established, but the mechanism of it is unclear. Dietary Na+ restriction reduces BP, and diuretics achieve a similar effect by depleting Na+ from the body. Diuretics can lower the blood pressure by 10-15 mmHg in most patients and are therefore adequate for mild or moderate hypertension.
For chronic treatment are thiazides and thiazide-like diuretics like hydrochlorothiazide, chlorthalidone, and indapamide the first choice.
For acute treatment of hypertension are loop diuretics like furosemide used.
Drugs that influence the sympathetic nervous system
In this category there are many drugs:
- Drugs acting on the vasomotor centre in the CNS
- Methyldopa
- Clonidine
- Drugs acting on α1 adrenergic receptors
- Prazosin
- Doxazosin
- Drugs acting on β adrenergic receptors
- Metoprolol
- Atenolol
These drugs work by either reducing periferal vascular resistance or decreasing the work of the heart, both of which reduce the BP according to the equation BP = CO x PVR.
Indications:
Centrally acting agents like methyldopa and clonidine are used in the treatment of hypertension during pregnancy, as they’re some of the few antihypertensives that aren’t teratogenic. They’re also second or third-line drugs in hypertensive crises.
Drugs blocking α1 adrenergic receptors like prazosin and doxazosin are used to treat hypertension due to phaeochromocytoma.
Drugs acting on β adrenergic receptors like metoprolol and atenolol are preferred to treat hypertension in patients who also have additional indication for β blockade, like angina or heart failure.
Mechanism of action:
Centrally acting agents stimulate the inhibitory α2 receptors in the vasomotor centre in the CNS. This decreases sympathetic outflow.
α1 blockers block catecholamine-mediated vasoconstriction. β blockers cause negative heart effects and decrease renin secretion.
Side effects:
Centrally acting agents:
- Sedation
- Depression
- Impotence
α blockers:
- Orthostatic hypotension
- Reflex tachycardia
β blockers:
- Bronchospasm
- Bradycardia
- Decreased peripheral circulation
- Hypertriglyceridaemia
Calcium channel blockers
These drugs reduce the Ca2+ influx into vascular smooth muscle and therefore decreases their tone. Recall from topic 1 that dihydropyridines are the only type that doesn’t also have cardiac effects.
Dihydropyridines may cause reflex tachycardia (which is bad for coronary artery disease) mostly just right after the beginning of the treatment. This is avoided when using sustained release (retard) preparations. They may also cause dizziness, flushing and peripheral oedema.
Dihydropyridines like nifedipine and amlodipine are preferred over non-dihydropyridines.
Potassium channel activators
These drugs activate ATP-regulated K+ channels. This causes hyperpolarization of vascular smooth muscle, which decreases their tone.
Minoxidil is the first type. It’s a prodrug that is converted into the active metabolite by a hepatic enzyme. It has the funny side-effect of causing hypertrichosis (excessive hair growth), which has led it to being used to treat baldness instead of hypertension. It is very rarely used as an antihypertensive nowadays, but is widely used to treat male pattern baldness!
Diazoxide acts exclusively on arterioles but also inhibits insulin secretion from β-cells. It acts very rapidly (within 30 seconds when given IV) and was therefore used for acute treatment of severe hypertension. It is not used anymore on this indication.
Drugs that increase cGMP
Sodium nitroprusside is an organic nitrate which releases NO when metabolized. NO activates intracellular soluble guanylyl cyclase, which increases intracellular levels of cGMP. This decreases the tone of vascular smooth muscle.
It also releases cyanide in small amounts when metabolized. This is normally not a problem but will be if overdosed or the person taking it has defective cyanide metabolism.
Sodium nitroprusside is used in cases where acute reduction of blood pressure is necessary, like hypertensive emergencies.
Drugs with unknown mechanism
Hydralazine is interesting as the mechanism of which it causes vasodilation is unknown. It significantly activates the sympathetic nervous system and should therefore always be used with beta blockers. It also frequently causes headache and nausea. It’s rarely used nowadays, only used as a second or third line in hypertensive emergencies and in hypertension in pregnant women.
Drugs acting on RAAS
Activation of RAAS increases the blood pressure by several mechanisms:
- Angiotensin II-mediated
- Generalized vasoconstriction
- Positive heart effects
- Increased sympathetic tone
- Stimulation of aldosterone
- Cell remodelling and hypertrophy of the myocardium
- Aldosterone-mediated
- Salt and water retention
You can read more about these drugs in topic 2.
ACE inhibitors and angiotensin receptor blockers are useful in treating mild-to-severe hypertension. They may notably be less effective in African Americans than in Caucasians as the former have lower plasma levels of renin than the latter.
Because RAAS is a slow-acting system the full BP-lowering effect is not seen until 3-6 weeks after the beginning of therapy.
What to use?
This is not important to know for the exam as the department doesn’t teach it. I’m including it because it obviously has clinical value and might clear up some confusion.
Like always we have the problem where there are so many drugs available and we don’t know which drugs to use when. According to the 2020 ISH guidelines for hypertension, combined treatment with two antihypertensive drugs in low dose (ideally in the same pill) is more efficacious and has less side effect than a single drug in a higher dose.
To determine which drug type to use should we keep the contraindications and potential side-effects of each drug type in mind. Some drugs also have other indications, and if the patient has these indications as well should we use that drug type. For example should patients suffering from both heart failure and hypertension be given ACE inhibitors or beta blockers as they are indicated for both conditions. Drugs affecting RAAS are contraindicated in pregnancy. Calcium antagonists should not be used in arrhythmias or heart failures. Beta blockers should not be used in asthma. Diuretics should not be used in gout.
If one drug type is unable to lower the BP satisfactorily is it recommended to add another type rather than to increase the dose of the first drug. This is to decrease the risk for side-effects.
2018 guidelines state that drugs like alpha blockers, centrally acting agents and aldosterone antagonists have too many side-effects to be considered as primary treatment for hypertension. These drugs can be considered if the hypertension can’t be controlled by the aforementioned drugs.
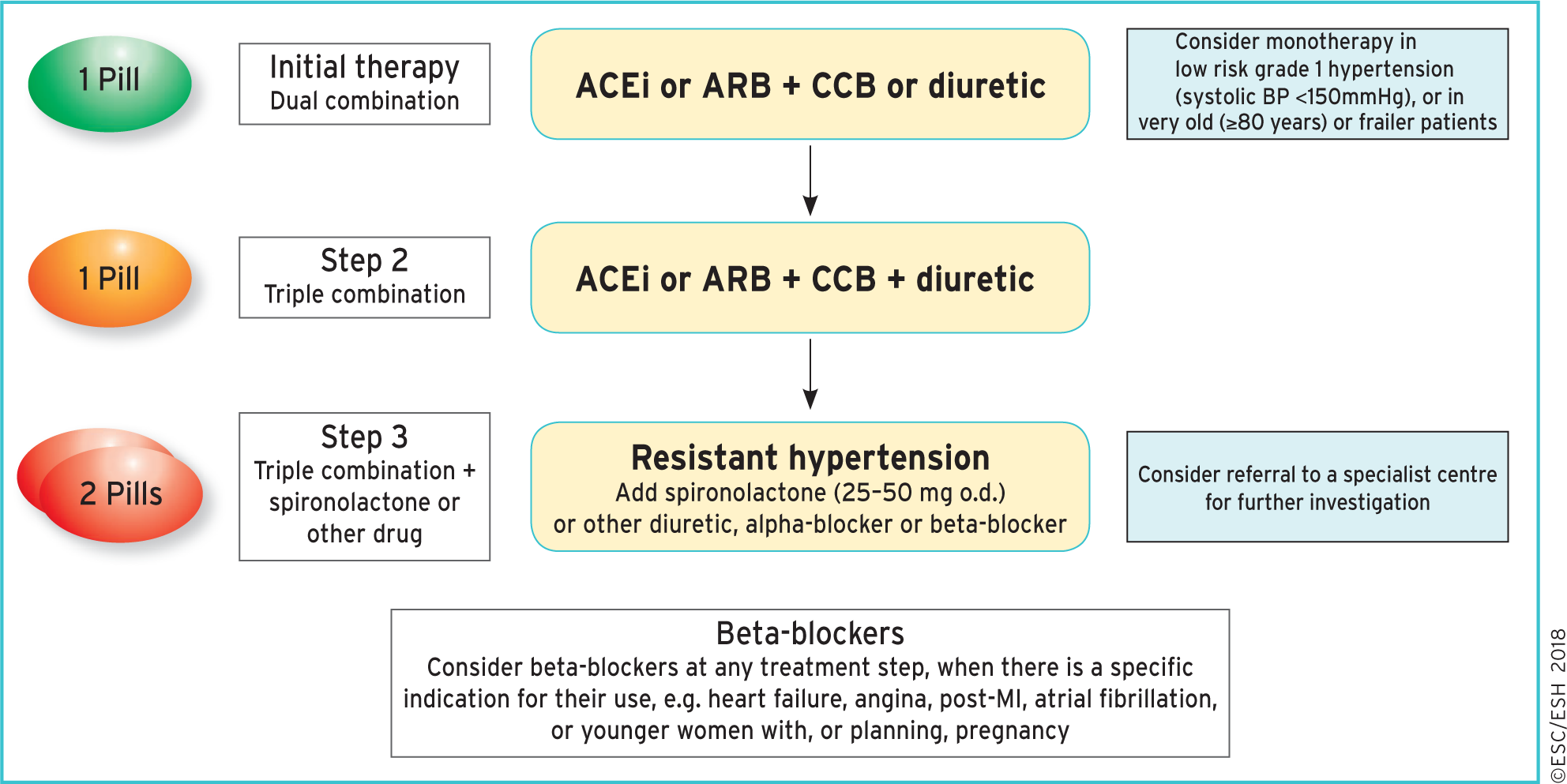
Drug treatment strategy for patients with hypertension and no other conditions. From https://academic.oup.com/eurheartj/article/39/33/3021/5079119#123461074. ARB = angiotensin receptor blocker. CCB = calcium channel blocker. ACEi = ACE inhibitor
Side effects of Methyldopa:
SIDE EFFECTS
Sedation, usually transient, may occur during the initial period of therapy or whenever the dose is increased. Headache, asthenia, or weakness may be noted as early and transient symptoms. However, significant adverse effects due to methyldopa have been infrequent and this agent usually is well tolerated.
The following adverse reactions have been reported and, within each category, are listed in order of decreasing severity.
Cardiovascular: Aggravation of angina pectoris, congestive heart failure, prolonged carotid sinus hypersensitivity, orthostatic hypotension (decrease daily dosage), edema or weight gain, bradycardia.
Digestive: Pancreatitis, colitis, vomiting, diarrhea, sialadenitis, sore or “black” tongue, nausea, constipation, distension, flatus, dryness of mouth.
Endocrine: Hyperprolactinemia.
Hematologic: Bone marrow depression, leukopenia, granulocytopenia, thrombocytopenia, hemolytic anemia; positive tests for antinuclear antibody, LE cells, and rheumatoid factor, positive Coombs test.
Hepatic: Liver disorders including hepatitis, jaundice, abnormal liver function tests (see WARNINGS).
Hypersensitivity: Myocarditis, pericarditis, vasculitis, lupus-like syndrome, drug-related fever, eosinophilia.
Nervous System/Psychiatric: Parkinsonism, Bell’s palsy, decreased mental acuity, involuntary choreoathetotic movements, symptoms of cerebrovascular insufficiency, psychic disturbances including nightmares and reversible mild psychoses or depression, headache, sedation, asthenia or weakness, dizziness, light-headedness, paresthesias.
Metabolic: Rise in BUN.
Musculoskeletal: Arthralgia, with or without joint swelling; myalgia.
Respiratory: Nasal stuffiness.
Skin: Toxic epidermal necrolysis, rash.
Urogenital: Amenorrhea, breast enlargement, gynecomastia, lactation, impotence, decreased libido.
And?
Hei!
“These drugs can have a strong BP-reducing effect but they have significant side-effects. Methyldopa is used to treat hypertension in pregnant women”
I have a feeling that its “no significant sides”? I mean since it is used in pregnant women
I changed that part slightly, but the thing that allows them to be used in pregnant women (despite side effects) is that they’re among the few antihypertensives that aren’t teratogenic. Also, one of the main side effects is impotence, which should affect pregnant women too much.