Page created on September 30, 2019. Last updated on December 18, 2024 at 16:57
Postmenopausal hormone replacement therapy
At menopause ovarian function decreases and oestrogen levels fall. This causes several problems, like osteoporosis, genital atrophy and increased cardiovascular risk, but also less severe problems like hot flushes, sweating, sleep problems, palpitation and mood disturbances. In theory, replacing oestrogen to postmenopausal women should eliminate all these problems. However, hormone replacement therapy is not without its own problems.
Hormone replacement therapy (HRT) has some benefits:
- It improves the less severe problems like hot flushes, sweating, etc
- Improves genital atrophy
- Prevents osteoporosis
However, it has several drawbacks:
- Giving oestrogen unopposed (without a progestin) increases the risk of endometrial cancer
- Giving oestrogen with a progestin increases the risk for coronary artery disease
- The risk for ovarian cancer increases
- The risk for breast cancer increases
- The risk for venous thromboembolism increases
- The risk for stroke increases
- The risk for gallstones increases
- The risk for risk for cardiovascular disease increases
In addition, there are better treatments for osteoporosis which have fewer drawbacks. Also, topical vaginal oestrogen preparations can be used to treat vaginal atrophy. For these reasons, few indications remain for systemic postmenopausal hormone replacement.
Indications:
Systemic postmenopausal hormone replacement therapy is indicated to relieve menopausal symptoms like hot flashes, mood alterations. It is not indicated in women with a history of breast cancer, coronary heart disease, previous thromboembolism or acute liver disease. Therapy should be started within 10 years of menopause, it should last for as short as possible and it should employ the lowest effective dose possible to decrease risks for complications.
However, according to recent studies and UpToDate, postmenopausal hormone replacement therapy is safe and suggested to women with moderate to severe menopausal symptoms who are within 10 years of menopause and who have to contraindications.
If the only symptom is vaginal atrophy, topical vaginal oestrogen preparations should be used instead of systemic treatment.
Choice of hormone and dosing:
Women with intact uterus (haven’t performed hysterectomy) should receive an oestrogen together with a progestin to prevent the increased risk for endometrial cancer. Women who have had a hysterectomy can receive oestrogen monotherapy.
The preferred oestrogen is estradiol. Oral micronized estradiol or transdermal estradiol is preferred.
The preferred progestin is oral micronized progesterone, but other progestins like norethisterone, levonorgestrel and medroxyprogesterone are options.
There are two ways to dose oestrogens and progestins. Oestrogen can be given alone for 15 days and then combined with progestin for 10 days, followed by a 5-day period of neither oestrogen nor progestin. During the 5-day period bleeding will occur. This dosing regimen corresponds to an artificial menstrual cycle.
The other way is to give oestrogen and progestin together every day. This causes endometrial atrophy and eventually stops menstrual bleedings completely.
Tibolone is a synthetic steroid with both oestrogen, progestin and androgen effects. It is quickly metabolized into three metabolites, each of these exert one of the aforementioned effects. It has oestrogenic effect on the vaginal mucosa and the skeleton, progestin effect on the endometrium and a positive effect on libido and mental wellness. However, it increases the risk of breast and endometrial cancer.
Hormonal contraception
Hormonal contraceptives involve the use of oestrogens and progestins to prevent pregnancy. Their efficacy is measured by the Pearl index. The Pearl index shows the number of unwanted pregnancies per 100 woman years.
Types:
Oral hormonal contraceptives exist in two forms. One is the combined pill, which includes an oestrogen and a progestin. The other type contains only a progestin, often called the minipill. The combined pill is the most efficacious, having a Pearl index of less than 1. The combined pill can also treat conditions like dysmenorrhoea, hypermenorrhoea, endometriosis and acne.
The oestrogen component is often ethinyl estradiol. The progestin component of the combination pill is often levonorgestrel, drospirenone or desogestrel. The progestin component of the minipill is often desogestrel, norethindrone or levonorgestrel.
Non-oral forms include transdermal patches, vaginal rings, intramuscular depot injection, intrauterine devices (IUD), subdermal implants and more. Medroxyprogesterone is given as an intramuscular depot injection.
The most common oral contraceptive by far is the combination pill. The minipill is usually only used in women who have contraindications for oestrogen-containing contraceptives.
Mechanism of action:
The exact mechanism of action depends on the type. The contraceptive effect of oestrogen and progestins is mainly mediated by negative feedback at the hypothalamus, which reduces the level of GnRH, which again reduces the release of FSH and LH from the pituitary. Without a surge in LH ovulation does not occur. Decreased FSH inhibits ovarian folliculogenesis.
In addition to the aforementioned hormonal effects, progestins have additional effects. It inhibits endometrial proliferation, increases the viscosity of cervical mucus and impairs fallopian tube peristalsis. These effects prevent sperm from reaching the egg, and they prevent the egg from implanting, should it be fertilized.
For progestin-only contraceptives the local effects in the uterus are more important for the contraceptive effect than the negative feedback effects.
Dosing schedules:
The classical dosing schedule of oral combined contraceptives is to take the drug for 21 days, and then to have a 7-day drug-free period during which a withdrawal bleeding occurs. The patient receives a pill blister pack with 28 pills. The first 21 pills contain the active ingredients while the last 7 are placebo.
Nowadays newer dosing schedules exist, where the drug is taken for longer than 21 days and with fewer and shorter drug-free periods, like 26 days with and 2 days without. This reduces the inconvenience associated with menstruation without causing any harmful effects.
For the combined contraceptives, monophasic and multiphasic preparations exist. In the monophasic preparations all pills in the cycle contain the same amount of active ingredients. In biphasic preparations, the pills in the latter half of the cycle contain more progestin than in the first half. Triphasic preparations also exist. Multiphasic preparations reduce the total cumulative amount of hormone taken. In theory this should reduce the number of adverse effects, however studies have not been able to demonstrate this. Thus, monophasic preparations are still preferred.
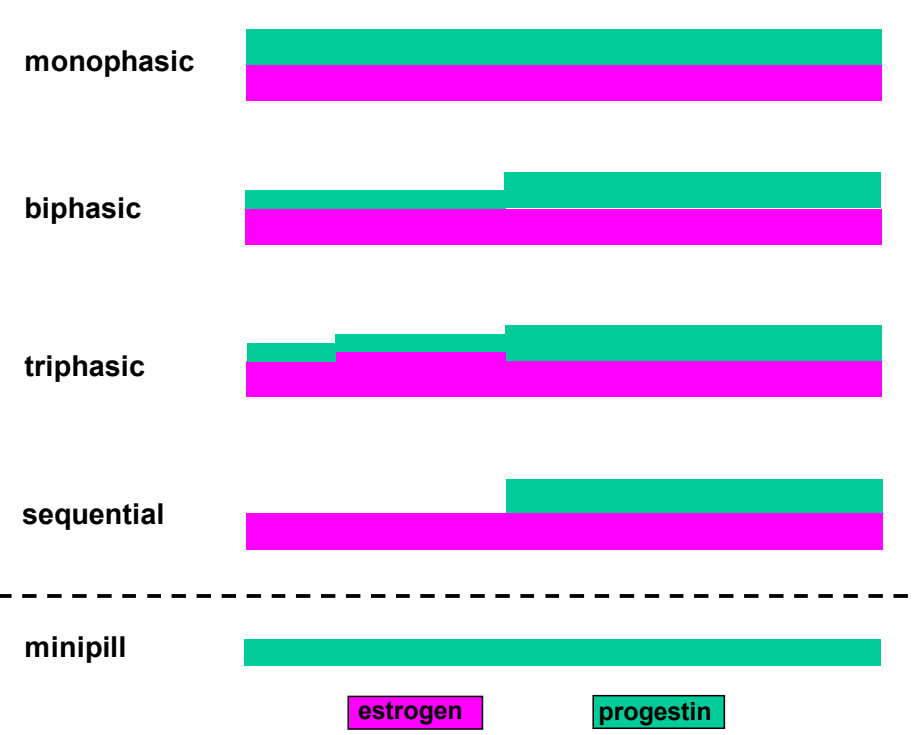
Illustration of the monophasic and multiphasic types of oral contraceptives. The x-axis shows time. The thicker the line the higher the dose of the active ingredient.
Progestin-only contraceptives should be taken continuously.
Comparison of combined and progestin-only contraceptives:
| Combined contraceptives | Progestin-only contraceptives | |
|
Effect on menstrual disorders |
Beneficial effect | No effect |
| Effect on endometriosis | Beneficial effect | No effect |
|
Effect on acne |
Beneficial effect | Unfavourable effect |
|
Risk of endometrial cc |
Reduced risk |
No change in risk |
|
Risk of ovarian cc |
Reduced risk | No change in risk |
|
Risk of colorectal cc |
Reduced risk |
No change in risk |
|
Risk of extrauterine pregnancy |
Reduced risk | No change in risk |
|
Effect on lactation |
Inhibition |
No effect |
| Effect on plasma triglyceride levels |
Increase |
No effect |
| Effect on gall stone formation |
Increase |
No effect |
| Risk of venous thrombosis |
Increase |
No change in risk |
|
Risk of arterial thrombosis |
Increase |
No change in risk |
|
Risk of hypertension |
Increase (mild) |
No change in risk |
|
Side effects like headache, mood changes, nausea, weight gain, decreased libido |
Yes |
Yes |
In conclusion, there is little reason to prefer the minipill for individuals with no contraindications for the combined contraceptive.
Contraindications for oestrogen-containing oral contraceptive:
- Cardiovascular
- Thromboembolism
- Coronary artery disease
- Hypertension (> 160/95)
- Metabolic
- Significant hypertriglyceridaemia
- Diabetes mellitus
- Oncologic
- Hepatic tumours
- Oestrogen-dependent tumours
- Smoking + >35 years of age
- Undiagnosed abnormal uterine bleeding
Emergency (postcoital) hormonal contraceptive
These drugs are meant to prevent pregnancy after intercourse. They’re most effective the sooner they’re taken after intercourse. They are not effective if taken later than 3 – 5 days after, depending on the type.
Common emergency contraceptives contain one of the following:
- Levonorgestrel 0.75 mg twice in 12 hours or 1.5 mg once
- Ulipristal (acetate) 30 mg
The Yuzpe regimen refers to when a person takes additional doses of their own oral combination contraceptive pills (containing levonorgestrel and ethinyl estradiol) as an emergency contraceptive. This method is less reliable than taking a dedicated emergency contraceptive.
The most efficacious and only non-hormonal emergency contraceptive is a copper IUD.
Mechanism of action:
Oral emergency contraceptives block or delay ovulation, but they do not inhibit fertilisation or implantation.
Ulipristal is a progesterone receptor partial agonist/antagonist. It’s effective up to 5 days after intercourse. Levonorgestrel is effective up to 3 days after intercourse.
Side effects:
A common side effect is nausea and vomiting. If vomiting occurs after taking the drug a new dose should be taken.
Special considerations:
For overweight and obese women levonorgestrel-containing emergency contraceptives do not give a significant reduction in pregnancy rate compared to when no emergency contraception is given. Ulipristal-containing emergency contraceptives are efficacious in overweight (BMI 25 – 30) women but it is 50% less efficacious in obese (BMI > 30) women.
In these populations a copper IUD should be used as emergency contraception instead. Copped IUD is also the only emergency contraceptive which is efficacious after ovulation has occured.
Hello Niklas, many thanks for the good write-ups. On the subject of emergency contraception, I would like to emphasize that they have been proven to work only before ovulation. I think this is a fact that is good for any future doctor (but also any adult ;)) to know. After ovulation, they cannot prevent fertilization. At least this is the current status. Uripristal has been discussed for years, whether it has other effects, but so far the researchers do not agree.
Hello! My name is Nikolas and not Niklas.
I’ll add a small note regarding this.
According to the lecture the hypertensive effect of combined contraceptives are negligible
Added
Correction: The Pearl index shows the number of unwanted pregnancies in 100 woman per year*
That is one interpretation of it, but it is defined according to woman-years. You can look it up.
Today, I went to the beach with my children. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear. She never wants to go back! LoL I know this is entirely off topic but I had to tell someone!
I don’t really understand how postmenopausal hormonal therapy and hormonal contraceptives made you think of this story, but cool.
Hiii,
“In biphasic preparations, the pills in the latter half of the cycle contain more oestrogen than in the first half“
According to the graph; in the 2nd half the pills contain more progestin
Good spot. fixed now.
So why can risk for ovarian cancer be increased with phrt,(which most likely is combined estrogen+progesterone) but the risk is reduced with combined hormonal contraceptives? Isn’t that contradicting..
That is a good observation, and it does seem contradictory, but it also seems to be correct. You can google it yourself. It might have something to do with the hormonal effect of stimulating ovulation in ovaries which have ran out of eggs (postmenopausal ovaries)? Who knows.
Hi 🙂 According to lecture, PHRT increases CV risk (also you listed increased risk for coronary A disease, which I suppose is CV disease?)
yes