Table of Contents
Page created on December 1, 2018. Last updated on December 18, 2024 at 16:56
Aneurysms
Introduction and types
Aneurysms are dilatations of blood vessels or of the heart which occur due to a weakness in the vessel wall. They may be congenital or acquired. We have several types which are easiest explained by this figure:
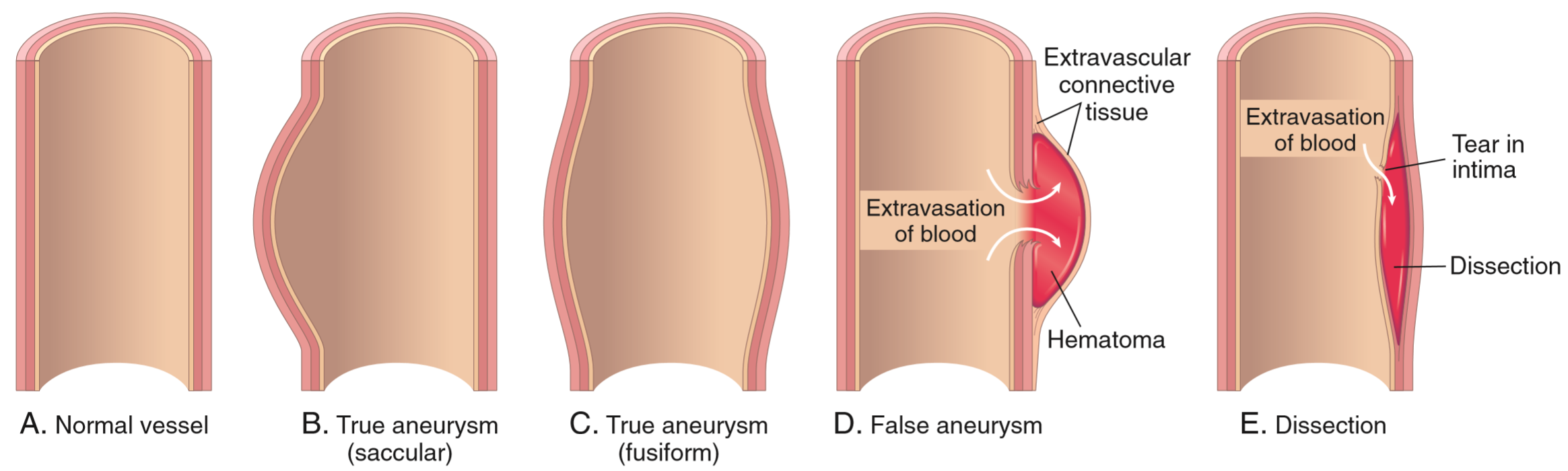
True aneurysms involve all three layers of the vessel. Saccular aneurysms are single-sided dilations, while fusiform aneurysms are circumferential dilations.
False aneurysms only involve extravascular connective tissue rather than the entire vessel wall. They occur due to the formation of a defect in the vessel wall, causing blood to extravasate, but rather than flowing out freely, the defect is retained by the extravascular connective tissue, in which a haematoma forms. From the outside, it may look like a saccular true aneurysm.
Aneurysms are dangerous primarily because they may rupture, but also because they may compress nearby structures. Tubrulence in the aneurysm also predisposes to the formation of thromboembolism.
Common locations and etiologies
Aneurysms occur due to a variety of disorders in a variety of locations. In most cases the underlying cause of a true aneurysm is either atherosclerosis or inflammation of the vessel wall (vasculitis).
- Aortic aneurysm – due to atherosclerosis, aortitis
- Coronary artery aneurysm – due to medium-vessel vasculitis
- Cerebral artery aneurysm – due to hypertension, connective tissue disease
- Carotid artery aneurysm – due to atherosclerosis
False aneurysms are more often the result of trauma, either accidental or iatrogenic.
Aortic aneurysms
Introduction
Aortic aneurysms are diseases of elderly with risk factors for atherosclerosis, like smoking, hypertension, and dyslipidaemia.
We distinguish two types of aortic aneurysms depending on the affected part of the aorta, thoracic aortic aneurysm (TAA) and abdominal aortic aneurysm (AAA). 90% of cases are abdominal. An aortic aneurysm is defined as a dilation > 50% of the normal diameter, or > 3 cm.
Abdominal aortic aneurysms (AAAs) occur in the abdominal aorta. They may be infrarenal (most common) or suprarenal. They usually start below the renal arteries and end above the iliac bifurcation. They can be saccular or fusiform, often with atherosclerotic plaques and large mural thrombi, like in our preparation. AAA are usually asymptomatic until they rupture.
Thoracic aortic aneurysms (TAAs) occur in the thoracic aorta. They are characteristic in hypertension, smoking, connective tissue disorders (Marfan, Ehlers-Danlos syndrome), and especially tertiary syphilis. It may cause symptoms of compression on other mediastinal structures, including:
- Dyspnoea – due to compression of the airways
- Dysphagia – due to compression of the oesophagus
- Cough – due to compression of the recurrent laryngeal nerve
Etiology
Risk factors for aortic aneurysms include:
- Hypertension
- Smoking
- Old age
- Tertiary syphilis
- Atherosclerosis
- Connective tissue disorders
Pathomechanism
The pathogenesis of aneurysms involves one or more of these factors:
- Abnormal wall structure due to genetic diseases
- Marfan syndrome
- Ehlers-Danlos syndrome
- Disturbed balance between collagen synthesis and degradation
- Recall from biochemistry that matrix metalloproteinases (MMPs) are enzymes that can break down connective tissue components like collagen, elastin, proteoglycans and so on.
- If MMPs are overexpressed will collagen in the arterial wall be degraded, which weakens the wall. MMPs are overexpressed by macrophages in atherosclerotic plaques and in vasculitis
- Smooth muscle cell loss or decreased ECM synthesis
- This can occur in ischaemic damage of tunica media in atherosclerosis or hypertension
- Metabolic causes
- Scurvy causes deficient collagen synthesis
- Blocking of the vasa vasorum
- End-arteritis in tertiary syphilis
Complications:
- Rupture of the aneurysm -> ischaemic stroke or hypovolaemic shock
- Mural thrombosis due to the turbulence inside the aneurysm
- Compression of nearby structures
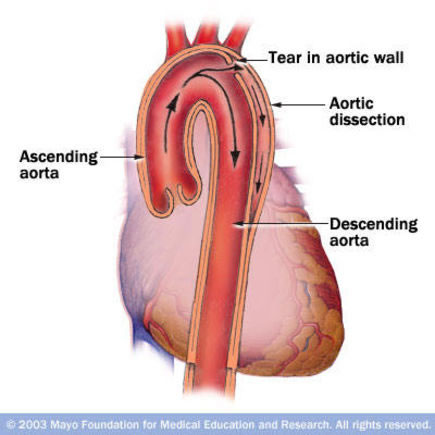
Aortic dissection
Arterial dissection occurs when there defect in the arterial tunica intima, leading to blood entering a virtual space between the tunica intima and tunica media. This forms a so-called false lumen inside this space. Unlike what the image at the top of the page shows, the false lumen may become larger than the true lumen. Blood may flow out of the false lumen through a second intimal tear.
The aorta is the artery most often affected by dissection. Aortic dissection is, like aortic aneurysm, mostly a disease of older men. It’s a quite deadly condition, with high mortality rate even with treatment.
Aortic dissection is problematic because it may rupture the aorta, or it may cause downstream ischaemia. If the dissection occurs above where a branching artery originates, the branching artery will no longer be supplied by blood from the true lumen but rather from the false lumen. Circulation in the false lumen is worse or non-existing, which may cause ischaemia of supplied tissues.
Etiology
The biggest risk factors for aortic dissections are:
- Hypertension (70% of patients have it)
- Atherosclerosis
- Connective tissue disease (Marfan syndrome, Ehlers-Danlos syndrome)
- Cocaine use
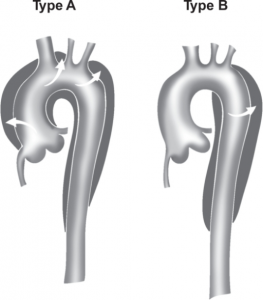
Classification
Two classification systems exist for aortic dissections, the Stanford classifications and DeBakey classifications, but the Stanford classification is the one which is used. Stanford type A aortic dissection originates from the ascending aorta and may extend all the way to the iliac bifurcation. Stanford type B aortic dissection originates from the beginning of the descending aorta and may also extend to the bifurcation. Stanford type A is the worst type.
Complications
- For both Stanford A and B
- Aortic rupture
- Bleeding (without complete rupture)
- Ischaemia of coeliac trunk, SMA, IMA
- Ischaemia of renal arteries
- Ischaemia of spinal arteries -> lower extremity weakness
- Exclusive for Stanford type A
- Ischaemia of coronary arteries -> acute myocardial infarction
- Ischaemia of carotids -> ischaemic stroke
- Aortic regurgitation
- Cardiac tamponade