Table of Contents
Page created on December 5, 2018. Last updated on December 18, 2024 at 16:56
Lung cancer
Introduction and epidemiology
Lung cancer is the second most frequent cancer, but it causes the most cancer-related deaths worldwide. Smoking is famously the biggest risk factor, and also the reason that lung cancer incidence increased dramatically during the 1900s. 85 – 90% of cases of lung cancer are attributable to smoking.
Around 95% of all primary lung tumors are carcinomas (epithelial origin), and these four types are most important:
- Non-small-cell lung cancer (NSCLC)
- Adenocarcinoma
- Squamous cell carcinoma
- Large cell lung carcinoma (LCLC)
- Small cell lung cancer (SCLC)
Non-small cell lung cancer (NSCLC) accounts for 85% of cases, while SCLC accounts for 15% of cases. Of the NSCLC, adenocarcinoma is the most common, followed by SCC and LCLC. SCLC is a neuroendocrine tumour.
Etiology
- Smoking
- Environmental exposure to carcinogens
- Radon gas
- Uranium
- Asbestos
- Polycyclic hydrocarbons
- Family history (Genetic susceptibility)
Smoking is by far the important cause of lung cancer, and it’s estimated that 90% of lung cancer cases would be avoided if not for smoking. Lung adenocarcinoma is not as strongly associated with smoking and is actually more common in nonsmokers than in smokers. The other types of lung cancer are very strongly associated with smoking.
We can compare smoking habits with a measure called “pack-year”. If you have smoked 1 pack of cigarettes (20 pcs) every day for one year you have accumulated 1 pack-year. If you smoke one half pack every day for four years you have accumulated 2 pack-years. This allows us to quantify smoking habits, and it has prognostic significance. Higher pack years means higher risk of smoking-induced cancer, as well as a poorer prognosis in the case of lung cancer.
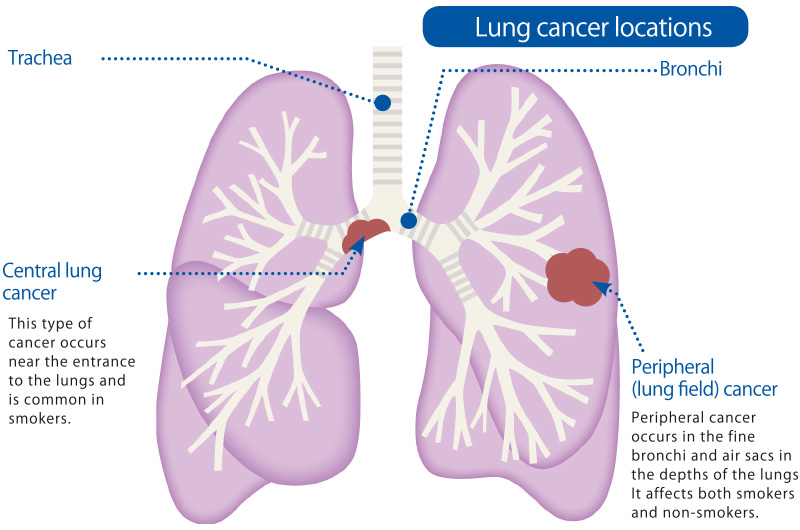
Localisation
The different types of lung tumors have a tendency to where they prefer to originate in the lung, either centrally or peripherally.
Centrally in this case means around the hilum and main bronchi. SCC and SCLC originate here. Central cancers usually cause symptoms earlier than peripheral cancers, because the cancers are closer to the airways. Central cancers also more frequently spread to surfaces like the mediastinum. It’s much harder to remove cancers surgically that are close to the bronchi without damaging the bronchi, so these cancers are much harder to treat surgically.
Peripherally in this case means anywhere else in the lung, often further away from the airways, often just beneath the pleural surface, subpleurally. Adenocarcinomas and LCLC originate here. These cancers will show symptoms at a much later stage than the central cancers, but they are also much easier to remove surgically.
Squamous cell carcinoma
SCC are found centrally, where they originate from major bronchi. Well-differentiated tumors will show keratinization, poorly-differentiated tumors won’t. It’s highly associated with smoking, but not with HPV, like laryngeal SCC is.
It follows the following process of development:
- Normal bronchial epithelium
- Basal cell hyperplasia
- Squamous metaplasia
- Squamous dysplasia
- Carcinoma in situ
- Invasive carcinoma
This development takes many years. The pathohistology slide shows this progression. These tumors usually form cavities because of central necrosis.
Adenocarcinoma
Adenocarcinomas are the most common type and are found peripherally. They’re the most common type in women and is less strongly associated with smoking. It’s strongly associated with several genetic mutations, like:
- EGFR (epidermal growth factor receptor)
- K-RAS
- ROS
- ALK/EML4
- PD-L1
These mutations are important because we have drugs which target the mutations specifically.
TTF-1 is a transcription factor that is expressed in lung adenocarcinomas and small cell carcinomas that is commonly used to distinguish between these types and squamous cell carcinoma, which doesn’t express TTF-1.
Neuroendocrine carcinomas
These cancers originate from neuroendocrine cells in the lung, cells that respond to nerve signals by producing endocrine hormones. They are also related to smoking. The grading system for neuroendocrine carcinomas is special; it’s dependent on the rate of mitosis in the tumor. The stages go like this:
| Stage | Rate of mitosis | Name | Prognosis |
| I | Slow | Carcinoid | Best prognosis |
| II | Atypical carcinoid | ||
| III | Fast | Large-cell lung carcinoma | |
| III | Fast | Small-cell lung carcinoma | Worst prognosis |
Small cell lung carcinomas (SCLC) are found centrally. They grow very quickly (have a very high turnover, tumour doubles every 50 days) and metastasize early. Because of this is surgery very rarely possible, however, thanks to the high turnover it responds well to chemotherapy. Because they grow so quickly, mitotic bodies are usually aplenty.
Large cell lung carcinoma is actually an umbrella term for a group of very poorly differentiated carcinomas, however one subtype, large cell neuroendocrine carcinoma, is neuroendocrine in origin. Large cell carcinomas are found peripherally.
Clinical features
Lung cancer usually spreads to:
- Hilar lymph nodes
- Mediastinum
- Pleura (pleural carcinosis)
- Brain
- Adrenal gland
Lymphangitis carcinomatosa may occur in the lung. It’s caused by the lymph vessels being filled up with invading malignant tumor cells. This causes the lymph vessels to dilate and become visible.
Symptoms of lung cancer include:
- Cough
- Haemoptysis
- Progressive dyspnoea
- Weight loss
Any lung tumor, regardless of subtype, is called a Pancoast tumor if it occurs in the apex of the lung. There are many structures in that area which the tumor can compress or invade, and so Pancoast tumors therefore have multiple extra consequences:
- Shoulder pain – due to compression of local nerve roots
- Pain in upper extremities – due to compression of the brachial plexus
- Horner syndrome – due to compression of the stellate ganglion
- Horner syndrome is a triad of miosis, ptosis, and facial anhidrosis
- Superior vena cava syndrome – due to compression of the SVC
- Dyspnoea
- Oedema of the face
- Hoarse voice – due to compression of the recurrent laryngeal nerve
Paraneoplastic syndromes are common in lung cancer, espacially in SCLC. Common occurrences include:
- ACTH secretion, leading to Cushing syndrome
- ADH secretion – leading to syndrome of inappropriate ADH (SIADH)
- Parathyroid hormone-related protein (PTHrP) secretion, leading to hypercalcaemia
- Dermatomyositis
- Acanthosis nigricans
Hi, I believe the sentence “lung adenocarcinoma is not associated with smokers” is a bit misleading. While in non-smokers, adenocarcinoma is by far the most common cancer of the lung, the majority of people diagnosed with adenocarcinoma are in fact smokers. Additionally, adenocarcinoma of the lung is strongly associated with cigarette smoking.
Thank you for clearing up something I’d apparently misunderstood.
Happy to! 🙂
I think the edited text is still a bit misleading though, as adenocarcinoma is in fact more common in smokers than in non-smokers. (see: https://en.wikipedia.org/wiki/Adenocarcinoma_of_the_lung#/media/File:Pie_chart_of_lung_cancers.svg) You might also want to change the text you missed to edit under “Adenocarcinoma”, ref: “.. is not associated with smoking”.
Uptodate states that adenocarcinoma is more common in never smokers than ever smokers, and I trust that source more than Wikipedia.
Thanks for the heads up on the section that I missed.
Would you share the source for that? I also use uptodate, but didn’t see that statement anywhere… I’d appreciate it!
(From the “lung cancer in never smokers” article, this is what I find: Adenocarcinoma is more common in never smokers, light smokers, and former smokers while squamous cell carcinoma and small cell lung cancer are seen with a higher incidence in heavy smokers, ref: https://www.uptodate.com/contents/lung-cancer-in-never-smokers?search=adenocarcinoma%20risk%20factors&source=search_result&selectedTitle=18%7E150&usage_type=default&display_rank=18 )
This article might also be relevant: https://academic.oup.com/aje/article/156/12/1114/151708?login=false#1252706
I’d be grateful if you could share which article you’re referring to!
In the summary of the same article it says “Adenocarcinoma is the most common pathology among never smokers and is more common than among ever smokers”.
This is by no mean to be stubborn, but I just had a desperate need to get to the bottom of this! The sentence in the summary does not reference to anything. In the pathology section it refers to, there are two articles that are referenced, none of which state that adenocarcinoma is more common in never smokers than in ever smokers. Both state that adenocarcinoma is the most common histological subtype of lung cancer in non-smokers, and that some mutations are more common in non-smokers than in ever smokers. Neither of them state that adenocarcinoma has a higher incidence in non-smoker than in ever smokers. At least not from skimming.
Sorry for having my mind stuck on this, lol
I’ve skimmed the literature, and I haven’t found any sources that state one or the other, other than the Uptodate summary. So I’ll trust the professors who wrote the article to have their facts straight.
Hey,
In the paraneoplastic changes what does AVP stand for?
Hey!
AVP stands for arginine vasopressin and is the modern name for the hormone you might know as anti-diuretic hormone (ADH).
I’ll update the description.