Table of Contents
Page created on May 20, 2019. Last updated on December 18, 2024 at 16:57
Consciousness
Consciousness is defined as “the capability of the individual to perceive and process environmental stimuli”. The state of consciousness can be characterised by:
- Its level, the state of wakefulness – the vigilance
- Its content – the integrity of the responses, the cognitive abilities
Vigilance is maintained by the ascending reticular activating system (ARAS) in the reticular formation in the brainstem and thalamus. This can be thought of as the degree of wakefulness and alertness.
The integrity of the consciousness is a function linked to the cortex, especially the prefrontal cortex. The cortex is responsible for producing meaningful responses to the stimuli perceived by the ARAS.
It’s important to distinguish these two aspects of consciousness as disorders can affect different aspects of it. For example, an individual can have normal vigilance, but the consciousness doesn’t produce meaningful responses to stimuli. On the other hand, a person can have decreased vigilance but normal integrity of the consciousness.
Disorders of vigilance
- Lethargy
- Somnolence
- Stupor
- Vegetative state
- Coma
- Brain death
- Pseudocomatous states
- Akinetic mutism
- Locked-in syndrome
Lethargy is a state of tiredness, weariness, fatigue or lack of energy. Motivation is decreased and spontaneous speech is rare but answering is normal. This is a normal state in sleep-deprivation or overexertion.
Somnolence is a state of abnormal sleepiness. The subject can still be aroused easily and answers normally. There might be a small delay before the person responds after being addressed.
Stupor is a state of insensitivity bordering on unconsciousness. The subject can only be aroused by strong stimuli. The subject may respond with short utterances after being aroused but soon falls back into an almost unconscious state. Painful stimuli will produce a defensive response.
A vegetative state is state of partial vigilance, but there is complete lack of cognitive function. It often occurs in people who wake up from comas. The subject may seem awake as their eyes may be open but there are no signs of awareness of the surroundings. There are no purposeful movements. All autonomic functions are normal; in fact, there are multiple cases where women in vegetative state have gotten pregnant and delivered healthy children.
Coma is a state of unconsciousness where there is no reaction to stimuli. We distinguish superficial and deep coma; in superficial coma a painful stimulus will produce a defensive response, in deep coma no response occurs. There are no ocular reflexes. Some autonomic functions may remain.
Brain death is a state where there is absolutely no evidence of brain function. There is no response to any stimuli, painful or otherwise, and there are no reflexes or spontaneous movements. No autonomic functions remain. An EEG will show no brain activity. Legally speaking, the patient is dead. By providing artificial life support the organs can be kept alive for transplantation.
Akinetic mutism is a coma-like state of limited responsiveness to the environment. The name implies that the person is unable to move (akinetic) or speak (mute), but this is not completely true. They can move and speak on their own initiative, but they will not do so if instructed.
Locked-in syndrome is a coma-like state where the consciousness is completely normal, but the subject cannot move any muscle or speak. Some of these patients can perform limited eye-movements.
Disorders of the content of consciousness
These patients are conscious, but their perception and evaluation of inner and outer stimuli is abnormal. It’s most frequent in psychiatric disorders, narcotics, hallucinogens or endogenous toxicosis.
- Misty consciousness
- Narrowed state of consciousness
- Confusion
Misty consciousness is a state where perception is decreased, and thinking is slow and not clear. It’s frequently seen just before falling asleep or just after waking up.
Narrowed state of consciousness is a temporary and transient state where the consciousness is restricted. This state can involve actions affected by poor judgement and can be thought of as “acting in the moment”. Examples include spontaneous murder or when you say something you didn’t intend to (a Freudian slip of the tongue). After the episode the person cannot give a good explanation of their actions, although they do remember them. Strong emotional response, depression, alcohol or drugs may be in the background.
Confusion is a state of partial or total disorientation in time and space. The vigilance is often reduced. Thinking is irregular and incoherent; the attention is constantly changing.
Integrative disorders of consciousness
These disorders are characterised by decrease of vigilance and abnormal content of the consciousness.
- Oneiroid state
- Tenebrosity
- Illusion
- Hallucination
- Delirium
An oneiroid state (from the Greek word “oneiros” = dream) is characterised by the subject being unable to judge what is real and what is not, like in a dream.
Tenebrosity is a state where the patient’s perception of the external world is abnormal. It involves delusions like illusions or hallucinations. An illusion is an abnormal perception of a real stimulus (seeing things as something other than what they really are), while a hallucination is an abnormal perception in absence of a real stimulus (seeing things that are not present).
Delirium is a state of impaired attention and cognitive function. Complete disorientation and incoherent thoughts occur. There may be alternating periods of relaxedness and agitation. The level of consciousness is fluctuating. There may be illusions and hallucinations. Amnesia after the episode is common.
Delirium can occur in virtually any disease, and especially in acute worsening of a disease. Polypharmacy, where a patient receives multiple medications, can cause delirium. It can also occur in alcohol or recreational drug use, as well as in severe fever.
Transient loss of consciousness
Transient loss of consciousness occurs in:
- Vasovagal syncope
- Transiently increased intracranial pressure
- Phaeochromocytoma
- Hypertensive crisis
- Epidural haematoma
- Head injury
- Epileptic fit
The Glasgow coma scale
The Glasgow coma scale (GCS) is a scale used to assess the state of a person’s consciousness. The person’s abilities in three categories are assessed and is given scores; the lower the score, the worse the condition. The scores in the three categories are summed and a total score is given. 3 is the worst possible score while 15 is the best possible score.
The three categories tested are eye response, verbal response and motor response. Points are awarded like this:
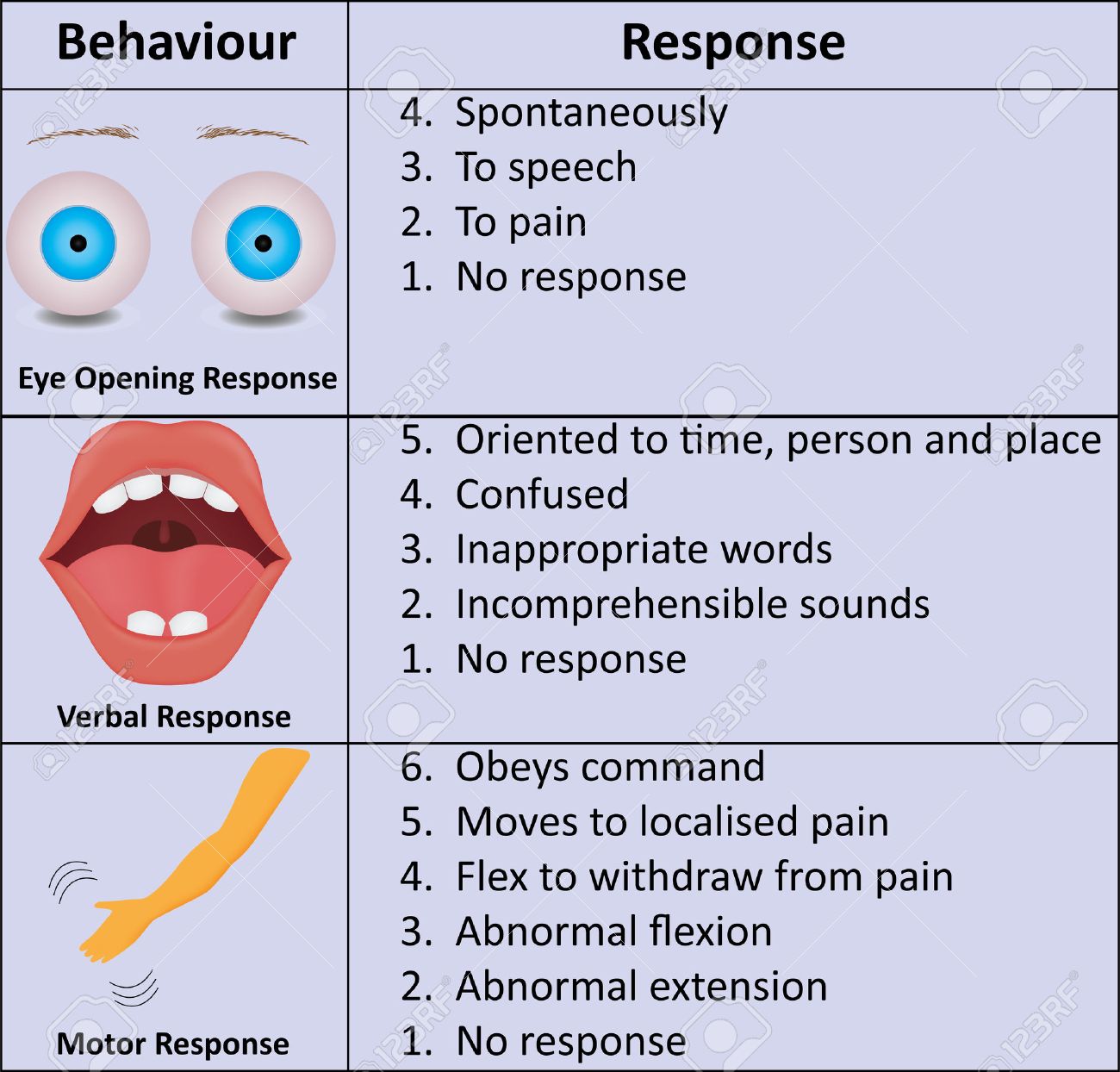
From https://www.123rf.com/photo_44288901_glasgow-coma-scale-gcs.html
Scores are evaluated like this:
- GCS score 13 – 15 – mildly decreased consciousness
- GCS score 9 – 12 – moderately decreased consciousness
- GCS score 5 – 8 – severely decreased consciousness
- GCS score ≤ 4 – high probability for lethal outcome
Causes of altered consciousness
- Disorders of circulation
- Ischaemia
- Hypoxia
- Hypoxaemia
- Anaemia
- Hypoglycaemia
- Exogenous toxins
- Drugs
- Toxins
- Heavy metals
- Cyanide
- Alcohol
- Recreational drugs
- Disorders of peripheral organ systems
- Hepatic encephalopathy
- Portal encephalopathy
- Uraemia
- Hyperglycaemic crisis
- Diabetic ketoacidosis
- Hyperglycaemic hyperosmolar syndrome
- Thyrotoxicosis
- Myxoedema coma
- Sepsis
- Electrolyte and pH disorders
- Disorders of sodium
- Acidosis
- Alkalosis
- Abnormal body temperature
- Heat stroke
- Hypothermia
- High fever
- CNS inflammation or infection
- Primary disorders of the CNS
- Epilepsy
Pathomechanism of coma development
One or more of the following mechanisms are usually involved in coma development:
- Decreased perfusion of the brain
- Decreased O2 supply to the brain
- Non-specific enzyme inhibition in brain cells
- Dysfunction of Na+/K+ ATPase -> increased intracellular Ca2+
- Development of false neurotransmitters
- Increased amount of inhibitory neurotransmitters
- Excitotoxicity
Excitotoxicity is a process where neurons are overstimulated by excitatory neurotransmitters like glutamate. These neurons take in too much Ca2+, which activates calcium-dependent enzymes that inhibit ATP production and cause DNA damage and potentially necrosis.
When the Na+/K+ ATPase dysfunctions, often due to ATP deficiency, the cell will compensate by activating a Na+/Ca2+ exchanger. This increases intracellular Ca2+, which causes damage by mechanisms explained above.
Alterations in intracellular osmolarity or pH causes the tertiary structure of proteins to slightly change, which slightly decreases their efficiency. This is the mechanism behind non-specific enzyme inhibition.
In the hyperglycaemic crises DKA and HHS osmotic diuresis causes hypovolaemia and therefore ischaemia of the brain. In DKA compensatory hyperventilation due to lactic acidosis contributes to this ischaemia by vasoconstricting brain vessels, while in HHS atherosclerosis is often present, which also decreases perfusion. The hyperglycaemia itself causes hypertonicity. Neurons produce idiogenic osmoles to prevent shrinking. These idiogenic osmoles non-specifically inhibit enzymes.
In hyperglycaemia the polyol pathway is highly active, which causes a state of pseudohypoxia. This decreases the production of ATP, leading to dysfunction of the Na+/K+ ATPase.
In hepatic and portal encephalopathy ammonia produced by enteric bacteria reaches the brain. Ammonia has multiple effects on the brain:
- It increases the permeability of the blood-brain barrier, allowing endogenous toxins to cross
- It inhibits the citric acid cycle, decreasing ATP production
- It causes stimulates the respiratory centre, causing hyperventilation and therefore brain vasoconstriction.
- It reduces levels of glutamate in the brain
Aromatic amino acids and GABA are normally metabolised by the liver, but in liver failure and portal hypertension they will reach the brain. The aromatic amino acids will be transformed into false neurotransmitters like phenyletanolamine and octopamine. These false neurotransmitters activate benzodiazepine receptors, which damages the neurons.
Mercaptans are by-products of intestinal bacteria breaking down sulphur-containing amino acids. They disturb the Na+/K+ ATPase.
In uraemic encephalopathy, many factors contribute to coma development:
- Uraemic toxins non-specifically inhibit enzymes
- PTH increases intracellular Ca2+
- Hyperosmolarity non-specifically inhibits enzymes
- Metabolic acidosis causes hyperventilation, which vasoconstricts brain vessels
- Anaemia occurs, causing anaemic hypoxia
- The glutamate level increases, causing excitotoxicity