Table of Contents
Page created on March 4, 2019. Last updated on December 18, 2024 at 16:57
Cirrhosis
Introduction and epidemiology
Cirrhosis is a chronic liver disease characterised by replacement of normal liver tissue by scar tissue. It’s an irreversible end-stage of hepatitis which cause significant morbidity and mortality. There is continuous loss of functional liver tissue, which is initially compensated and asymptomatic as the remaining liver can compensate. However, acute insults precipitate decreases in liver function, causing hepatic decompensation and development of dramatic and life-threatening complications. Cirrhosis is also an important risk factor for hepatocellular carcinoma.
Cirrhosis is a common condition worldwide.
Etiology
- Alcoholic liver disease
- Metabolic associated fatty liver disease
- Chronic viral hepatitis (C, B or D)
- Haemochromatosis
- Biliary obstruction (primary biliary cholangitis, primary sclerosing cholangitis)
- Autoimmune hepatitis
- Wilson’s disease
- Heart failure
- Alpha-1 antitrypsin deficiency
The most common causes are alcoholic liver disease and hep C infection.
Pathology
Continous necrosis and regeneration of the liver parenchyme replaces the functioning liver parenchyme with fibrosis. The pattern of fibrosis eventually forms fibrous septa. The more prominent they become, the more the liver takes on a nodular cirrhotic appearance. Histology shows pseudolobules separated by fibrosis. These pseudolobules can be distinguished from hepatic lobules by the fact that they don’t have a central vein.
The liver will now be a brown, shrunken, nonfatty organ composed of cirrhotic nodules.
We can distinguish multiple types of cirrhosis:
- Micronodular cirrhosis (Laennec cirrhosis) – caused by alcoholism
- Macronodular cirrhosis – caused by chronic hepatitis B or C or by autoimmune hepatitis
- Pigment cirrhosis – Caused by hemochromatosis (iron accumulation) or Wilson disease (copper accumulation)
- Biliary cirrhosis – Caused by damage to the biliary tree
Clinical features
Cirrhosis causes hepatic failure, the symptoms of which you can read about below, but the most significant are jaundice, ascites, and hepatosplenomegaly. Laboratory findings in cirrhosis show:
- Elevated serum aminotransferases (ALT and AST) and alkaline phosphatase
- Hyperbilirubinemia,
- Hypoproteinaemia (globulins, albumins and clotting factors)
- Anaemia
- Elevated INR – due to decreased production of clotting factors
Hepatic failure
Introduction
Hepatic or liver failure, also called hepatic decompensation, describes the condition where the liver is unable to perform its normal functions. This occurs because the liver parenchyme is so damaged or replaced by scar tissue that the remaining liver cannot compensate for the loss. It may be acute or chronic, but chronic is much more common. Chronic hepatic failure is almost synonymous with cirrhosis, as cirrhosis is the most common cause.
Etiology
- Acute hepatic failure
- Acute viral hepatitis (A, E)
- Drug effects
- Poisonous mushrooms, phosphorous, CCl4 and halothane
- Paracetamol overdose
- Chronic hepatic failure (cirrhosis)
Complications
The complications of hepatic failure are many, and it can be divided into two types:
- Parenchymal decompensation – due to decreased function of the parenchyme
- Hypoproteinaemia
- Hypoalbuminaemia -> oedema, ascites
- Decreased production of clotting factors -> coagulopathy -> excessive bleeding
- Hyperbilirubinaemia -> jaundice
- Hepatic encephalopathy -> confusion and altered mental status
- Hepatorenal syndrome
- Hepatopulmonary syndrome
- Hypoproteinaemia
- Vascular decompensation – due to congestion of the portal circulation
- Ascites
- Portal hypertension
- Oesophageal varices -> can cause significant bleeding
- Caput medusae
- Splenomegaly
- Malabsorption
You can read more about these consequences in pathophysiology 2.
Alcoholic liver disease
Alcoholic liver disease and non-alcoholic fatty liver disease don’t have their own topics, but they’re important disorders to know.
Introduction and epidemiology
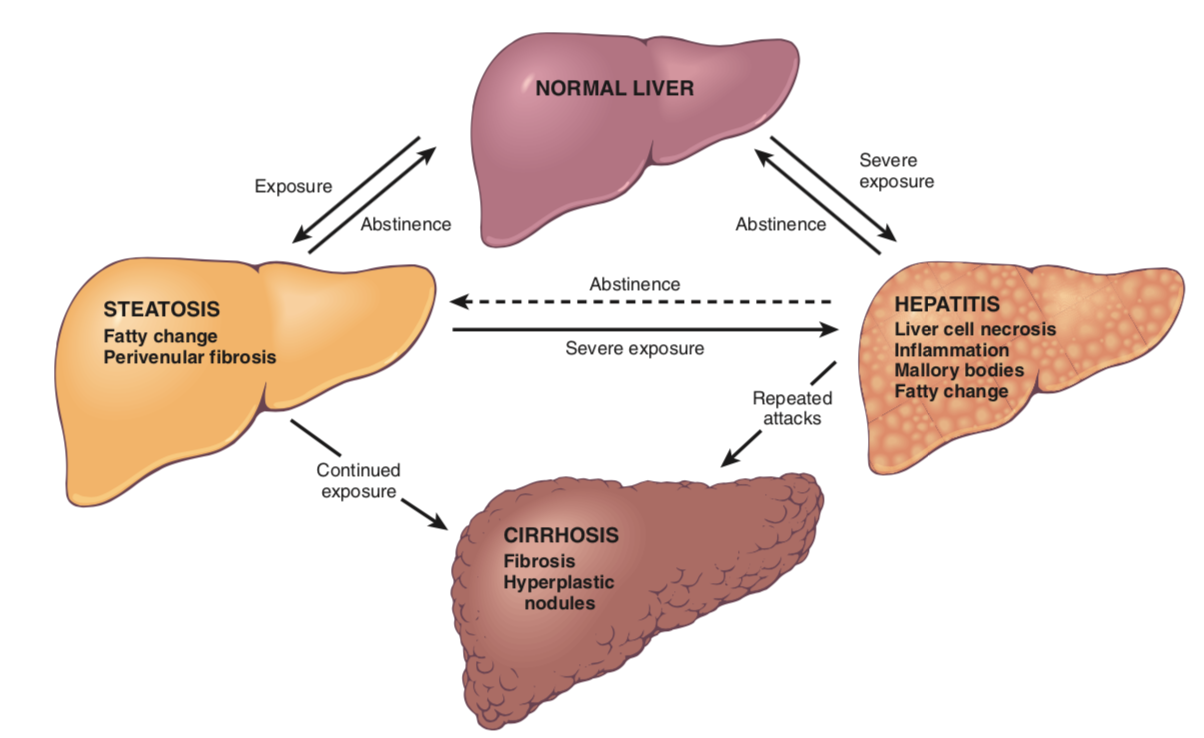
Alcoholic liver disease (ALD) is an umbrella term for liver conditions caused by significant and chronic alcohol abuse. It initially causes liver steatosis, which progresses to alcoholic hepatitis to cirrhosis unless alcohol consumption stops.
Almost all who abuse alcohol develop liver steatosis, which is reversible, but only a few progress to hepatitis and cirrhosis. Hepatitis C is often found in chronic alcoholics and leads to acceleration of alcoholic liver disease.
Excessive ethanol consumption causes more than 60 % of chronic liver diseases in the Western countries and is the 5th leading cause of death. Alcoholic liver disease is a major cause of liver transplantation.
Etiology
Alcoholic liver disease is caused by significant alcohol consumption over long periods of time. The risk increases proportionally with the amount of alcohol consumed. There is no threshold above which ALD invariably develops, as this varies from person to person, but most people with ALD have been drinking ~10 units daily for decades.
When talking about alcohol consumption, it’s important to define how much a unit of alcohol is. In Europe in general, one unit is 10 g of alcohol, while it’s 14 g in the US. This corresponds to one 0,33 L beer, one glass of wine, or one small glass of hard liquor.
Some “fun facts” about alcohol drinking: women are more susceptible to alcohol-induced liver injury, and binge drinking may be as harmful as daily drinking.
Pathomechanism
Hepatocellular steatosis results from shunting substrates away from catabolism and towards lipid synthesis, because alcohol dehydrogenase generates so much NADH from all the ethanol that lipid synthesis is favoured by the metabolism. You can read more about this pathophysiology 2.
The causes of alcoholic hepatitis are most likely toxic products and metabolites from ethanol metabolism, like:
- Acetaldehyde
- Reactive oxygen species generated during oxidation of ethanol
- Cytokine-mediated inflammation and cell injury
- Alcohol itself
The progression of alcoholic liver disease is as follows:
- Hepatocellular steatosis
- Steatosis refers to fatty change of the liver. Fat accumulates in the hepatocytes, and the centrilobular ones are the first ones to acquire this change. The lipid accumulation in hepatocytes spreads outward from central veins to the midlobular and periportal hepatocytes. The lipid droplets that accumulate expand the cells and displace the nucleus.
- Macroscopically, the liver is very big (4-6 kg or more), soft, yellow and greasy.
- Steatohepatitis
- Steatohepatitis refers to the presence of both inflammation and steatosis.
- Hepatocyte ballooning, where single or scattered foci of hepatocytes undergo swelling and necrosis.
- Mallory-Denk bodies, which consists of damaged intermediate filaments, and can be seen as very eosinophilic inclusion bodies in degenerating hepatocytes
- Neutrophil infiltration – neutrophils accumulate around the degenerating hepatocytes. Especially around the Mallory-Denk bodies.
- Cirrhosis
- A distinctive pattern of scarring occurs. It appears first as central vein sclerosis, and spreads outwards, encircling individual or small clusters of hepatocytes. It looks like a chicken wire fence in the microscope.
The area around the central veins are most susceptible to toxic injury because the generation of acetaldehyde and free radicals is biggest there. Pericellular and sinusoidal fibrosis develop in this area as well. Both steatosis and alcoholic hepatitis can be reversible if the patient stops drinking alcohol.
Alcohol-induced liver damage usually has an increased AST/ALT ratio on labs, commonly higher than 2.
Metabolic associated/non-alcoholic fatty liver disease
Introduction and epidemiology
Metabolic associated fatty liver disease (MAFLD), previously known as non-alcoholic fatty liver disease (NAFLD), refers to liver disease which develops due to obesity and diabetes mellitus type 2. The pathology and progression is similar as with ALD, but there is no alcohol abuse involved. It progresses similarly as ALD, from steatosis to non-alcoholic steatohepatitis (NASH) to cirrhosis.
Recently (2020), it’s been proprosed that NAFLD needs a new name to better describe its pathogenesis, namely metabolic associated fatty liver disease (MAFLD).
It’s a very common condition in the Western world.
Pathomechanism
Insulin resistance results in accumulation of triglycerides in hepatocytes due to these mechanisms:
- Impaired oxidation of fatty acids
- Increased synthesis and uptake of fatty acids
- Decreased hepatic secretion of VLDL cholesterol.
The fat-loaded hepatocytes are very sensitive to lipid peroxidation products generated by oxidative stress, which can damage mitochondria and plasma membranes. This leads eventually to apoptosis of the hepatocytes. A consequence of oxidative stress or release from visceral adipose tissue is that the levels of TNF and IL-6 increase, contributing to liver damage and inflammation.
Hello! Just wanted to let you know that on the lecture it is written that hepatic failure leads to hyperglobulinaemia, not hypo! I was confused, so I asked my teacher about it, and she explained it like this:
The liver synthetizes the albumin, and since it is incapable, there is hypoalbuminaemia. The globulins are mostly from the immunoglobulins and the liver is an important site of immunoglobulin catabolism. In liver failure liver cannot do this, and lots of the globulin fraction remains circulating in the blood.
Changed,
Cheers
hi greek doctor, can you please explain about HEPATIC STEATOSIS and ALCOHOLIC HEPATAITIS?
i,m confused. are they the same or totally different things? is there a connection between them (e.g one can progress to another) .
which one is more dangerous?
also , STEATOHEPATATIS and HEPATIC STEATOSIS , do they have the same meaning or not?
thanks.
Steatosis is another word for fatty change. Hepatic steatosis refers to fatty change of the liver. Many things can cause hepatic steatosis, including alcohol consumption and metabolic syndrome. In fact, steatosis is visible in healthy people after binge-drinking, but is then of course completely reversible.
Alcoholic hepatitis refers to actual inflammation of the liver. It is a later stage of hepatic steatosis which occurs in long-term alcohol abuse. Alcoholic hepatitis may be reversible, but it may also progress into alcoholic cirrhosis.
Steatohepatitis refers to the presence of inflammation (hepatitis) at the same time as steatosis. The term is used to distinguish hepatitis where steatosis is present (like NASH and alcoholic hepatitis) from hepatitis where steatosis is not present (like viral hepatitis).
you,re a life saver,
you rock more than the rock himself. <3
What an honour <3