Table of Contents
Page created on April 22, 2019. Last updated on December 18, 2024 at 16:57
General
Testicular cancer is most frequent in young males. It is the most common tumor in men in the 15 – 35 age group. There are 6 – 8 new cases per 100 000 every year in Hungary. There are three age peaks where testicular cancer is most common:
- 15 – 35 years (the most common age group)
- 0 – 10 years
- > 60 years
Common risk factors include:
- Cryptorchidism
- Previous testicular cancer
- Positive family history
- Gonadal dysgenesis
- Klinefelter syndrome
- Down syndrome
96% of all testicular tumors are malignant. Despite this the prognosis is excellent. Even advanced and metastatic testicular cancers are often curable.
Testicular tumors usually present as firm, painless masses on the testis. Unlike hydroceles, these masses cannot be transilluminated. Ultrasound may yield more information about the mass. Testicular masses are never biopsied, which is the normal procedure for suspected tumors elsewhere in the body. Instead, sperm is cryopreserved, and the testis is removed by orchiectomy. Because the vast majority of testicular tumors are malignant there is a high chance the testis would have been removed anyway. Also, biopsying a malignant testicular tumor could allow tumor cells to seed in the scrotum. These are the reasons biopsies of the testis are never performed.
AFP and hCG are important tumor markers in testicular tumors. Different histological subtypes have different patterns of expression of these tumor markers.
95% of testicular tumors originate from germ cells. The remaining 5% originate from the testicular stroma (which is derived from the sex cords), including Sertoli cells, Leydig cells or granulosa cells.
The classification can be visualised like this:
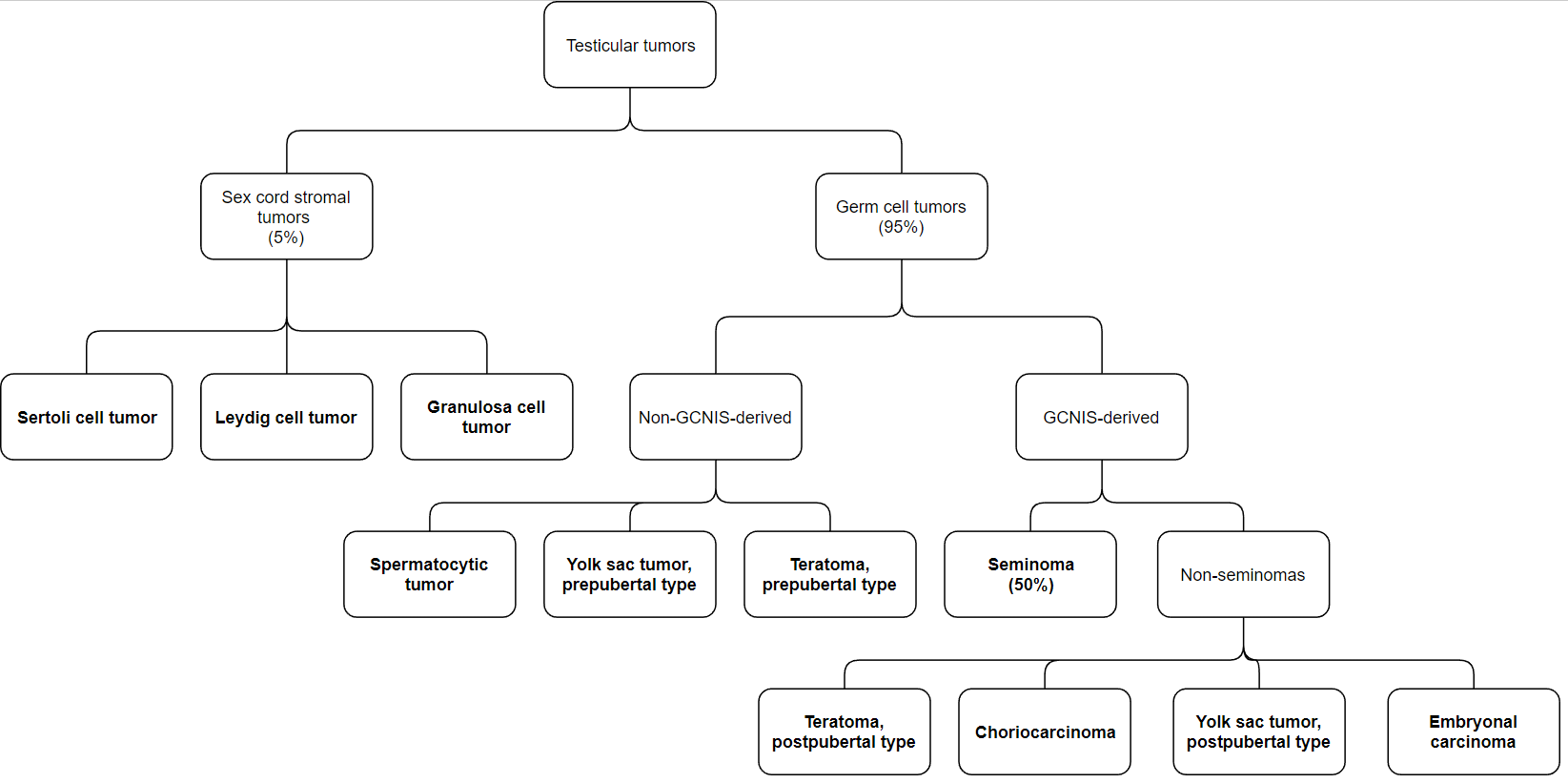
Germ cell tumors
Germ cell tumors develop from totipotent germ cells. During embryonal development these totipotent cells can travel down normal differentiation pathways and become spermatocytes. However, if they instead travel down abnormal developmental pathways, they can become seminomas or embryonal carcinomas. Embryonal carcinoma cells can then take one or more of these courses: They can undergo (intra)embryonic differentiation and form a (postpubertal) teratoma (which is comprised of embryonic tissues). They can undergo extraembryonic differentiation and form (postpubertal) yolk sac tumors or choriocarcinomas (which are extraembryonic tissues). Lastly the totipotent germ cells can remain undifferentiated and remain embryonal carcinoma. This is better illustrated on the figure below:
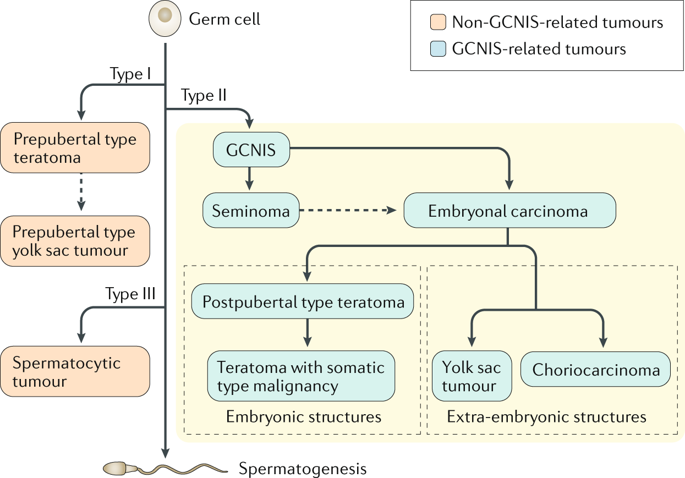
From https://www.nature.com/articles/s41572-018-0029-0. I don’t think this is very important to know but it might impress the examiners.
Germ cell tumors account for 95% of all testicular tumors. It’s very common (in 60% of cases) for germ cell tumors to contain more than one histological subtype. These are called mixed germ cell tumors. The remaining 40% of cases are pure germ cell tumors and contain only one histological subtype.
Most germ cell tumor develop from a precancerous lesion called germ cell neoplasia in situ (GCNIS). This precancerous lesion is virtually always present together with the mature GCNIS-derived germ cell tumor when examined histologically. This lesion has a 50% chance of progressing into cancer within 5 years.
Isochromosome 12p or extra copies of 12p is seen in almost all germ cell tumors.
GCNIS-derived germ cell tumors
Seminoma is the most common pure testicular germ cell tumor. It most frequently occurs in patients in their 40s. Seminomas grow slowly and rarely metastasize, and therefore have a better prognosis than non-seminomas. It also has a good radiosensitivity, meaning that it’s highly treatable by irradiation. Seminomas are homogenous masses with small foci of haemorrhage or necrosis. Some cases of seminoma can produce hCG.
Non-seminomas don’t respond as well to treatment as seminomas, and they metastasize earlier.
Embryonal carcinoma is most frequent in the 20 – 30-year age group. It frequently metastasizes. It’s most frequently found as a component of mixed germ cell tumors and is rarely found in pure form. The cells resemble primitive, embryonal cells and are therefore rapidly growing, often forming haemorrhage or necrosis.
Yolk sac tumor exists in two forms: the prepubertal type and the postpubertal type. In both forms the totipotent germ cells undergo extraembryonic differentiation and become yolk sac cells. Like the physiologic yolk sac, these tumors produce AFP (alpha-fetoprotein). The prepubertal form is the most common of the two. Structures resembling primitive glomeruli can be seen histologically, the so called Schiller-Duval bodies.
The postpubertal yolk sac tumor is a non-seminoma and is most frequently seen in adult mixed tumors. In the postpubertal type hemorrhage and necrosis is common.
Choriocarcinoma most frequently occurs in the 20 – 30-year age group. As the name implies, this tumor is formed when totipotent germ cells undergo extraembryonic differentiation and become placental cells. It’s the most aggressive type of testicular cancer, and therefore metastasizes very early and therefore often presents with symptoms of lung and brain metastases. Like the placenta this tumor produces hCG, so this tumor marker will be elevated. According to Dr. Bela this type also may contain foci of necrosis and hemorrhage.
Teratoma exists in two forms: the prepubertal type and the postpubertal type. In both forms the totipotent germ cells undergo (intra)embryonic (= somatic) differentiation and form somatic tissues from one or more germ layers. While teratomas are benign in females, they are malignant in males.
The postpubertal teratoma develops from GCNIS. It’s commonly found as a component of mixed germ cell tumors. It is malignant, unlike the prepubertal teratoma.
Mixed germ cell tumors account for 60% of all germ cell tumors, and as such most testicular tumours are mixed. They frequently produce AFP and/or hCG. These are the most frequent combinations:
- Embryonal carcinoma + seminoma
- Embryonal carcinoma + teratoma
- Embryonal carcinoma + teratoma + yolk sac tumor
Non-GCNIS-derived germ cell tumors
Spermatocytic tumor (also called spermatocytic seminoma) occurs most frequently in older men. It develops from spermatogonia, a post-pubertal germ cell, which explains why it only occurs in older men. It does not derive from GCNIS. It rarely metastasizes.
The prepubertal yolk sac tumor is the most common testicular tumor in children; the mean age upon diagnosis is 3 years old. This type is almost always pure. AFP is elevated.
The prepubertal teratoma is the second most common testicular tumor in children. Unlike most germ cell tumors it does not have isochromosome 12p. Contrary to the name it may also occur in adults, where it accounts for 20% of all teratomas. Prepubertal teratoma is benign, unlike the postpubertal type.
Sex cord stromal tumors
These tumors account for 5% of all testicular tumors in adults, but they are much more frequent in childhood. These tumors arise from Leydig cells, Sertoli cells or granulosa cells. They are usually benign.
Leydig cell tumors may produce testosterone, which can cause early puberty in children. Occasionally they can cause symptoms of femininization as well.
Lymphoma
Lymphomas may occur in the testes as well, most frequently as diffuse large B-cell lymphoma (DLBCL). These are the most frequent testicular tumors in men older than 60.
Summary
| Tumor | Peak patient age | Tumor marker status | Important characteristic |
| Seminoma | Middle-aged adults (40 – 50) | 10% produce hCG | Good response to irradiation. Never necrotic. |
| Embryonal carcinoma | Young adults (20 – 30) | No tumor markers | Metastasize early. Necrotic and haemorrhagic tumor. |
| Choriocarcinoma | Young adults (20 – 30) | Produce hCG | Metastasize very early, most aggressive type |
| Mixed germ cell tumor | Young adults (15 – 30) | Produce hCG or AFP | Almost always includes embryonal carcinoma |
| Yolk sac tumor | Young children (< 5) | Produce AFP | Prepubertal type |
| Teratoma | All ages | No tumor markers | Benign if prepubertal type, malignant if postpubertal type |
| Spermatocytic tumor | Older adults (> 60) | No tumor markers | |
| Lymphoma | Older adults (> 60) | No tumor markers | Usually DLBCL |
Hi you have written seminoma is the most pure why it is written with embryonal cell in a mixee combination
Seminoma is the most common tumour which is not mixed, but it can also be a component of mixed tumour. Mixed tumours are more common than pure seminomas.
Have you ever thought about including a little bit more than just your articles? I mean, what you say is fundamental and all. However think of if you added some great pictures or video clips to give your posts more, “pop”! Your content is excellent but with images and clips, this blog could undeniably be one of the best in its niche. Fantastic blog!
Hey Meaghan
I’m not sure adding pictures or video clips of testicular tumours would be a good suggestion, or that the post needs more “pop”.
hi greek doctor,
for tumors that are haemorrhaic or necrotic , dr.bela said that choriocarcinoma and yolk sac tumor, also cause them as well.
thought it could help mentioneding it to you . cheers brother.
Fixed.
Cheers!
Added, thank you.
hi greek doctor,
for tumors that are haemorrhaic or necrotic , dr.bela said that choriocarcinoma and yolk sac tumor, also cause them as well.
thought it could helptelling it to you . cheers brother.
Hello Nick ❤️
Regarding seminoma the Robbin’s mentioned that large tumors may contain foci of coagulation Necrosis, usually without hemorrhage. P660
Some sources say necrosis without haemorrhage, some say both, some say neither..
Fixed.