Page created on May 23, 2019. Last updated on December 18, 2024 at 16:56
I recommend reading through topic 4 of internal medicine for a better introduction to this topic.
Introduction
In pre-excitation syndromes an accessory conducting fibre is present. This accessory fibre bypasses the normal conduction system and therefore allows the ventricles to be depolarized earlier than normal.
There are two important types:
- Wolff-Parkinson-White syndrome
- Lown-Ganong-Levine syndrome
Wolff-Parkinson-White syndrome
In Wolff-Parkinson-White syndrome (WPW) an accessory conducting fibre is present between the atria and ventricles. This fibre is called the “bundle of Kent”. The bundle of Kent bypasses the AV node and allows signals to travel directly from the atria to the ventricles without passing through the AV node. The AV node usually delays the signal. This delay is avoided in WPW.
The bundle of Kent can be present in the left ventricle or in the right ventricle. These accessory fibres are fast-conducting and have short refractory time.
Symptomatic patients with WPW develop episodes of a type of paroxysmal supraventricular tachycardia called atrioventricular re-entry tachycardia (AVRT).
Less than 0.3% of the population is affected. Around 40% of those with the condition never develop symptoms.
Etiology:
It’s unknown what causes the appearance of the bundle of Kent. It’s a congenital condition. There might be hereditary factors.
ECG morphology:
- PQ-interval decreased (< 120 ms)
- Delta-wave is present
- QRS is wide (> 120 ms)
- Secondary repolarization disorders
Because the ventricles are depolarized earlier than normally, the QRS complex occurs earlier after the P-wave than normally.
The delta-wave is a small upstroke on the beginning of the QRS complex. It occurs as the impulse travels through the myocardium after passing through the bundle of Kent. The delta waves can be present in different leads depending on which ventricle the bundle of Kent is present in.
The QRS complex is wide as it begins earlier than normal and ends at the normal time.
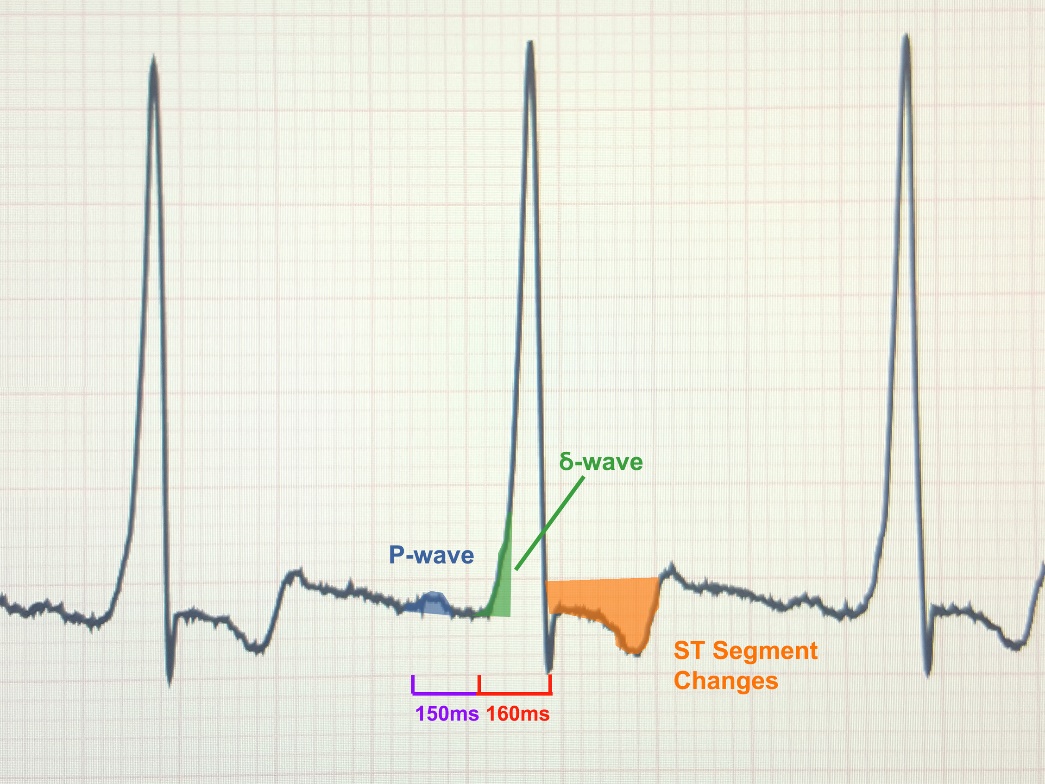
From https://jetem.org/asymptomatic_wpw/
Clinical features:
Symptomatic patients with WPW develop episodes of a type of paroxysmal supraventricular tachycardia called atrioventricular re-entry tachycardia (AVRT). These episodes are characterised by palpitations, dizziness, chest pain, dyspnoea and potentially syncope.
These episodes can be triggered by stress or exertion, but they can also occur randomly.
Any atrial impulse will be transmitted to the ventricles through the bundle of Kent, so atrial fibrillation or flutter will cause life-threatening ventricular arrhythmias like ventricular tachycardia or fibrillation.
Treatment:
Episodes of paroxysmal supraventricular tachycardia should be treated with carotid massage or Valsalva manoeuvre, to increase the parasympathetic tone.
The bundle of Kent can be burnt off with catheter ablation if it causes symptoms. Medical treatment is also available.
Lown-Ganong-Levine syndrome
Lown-Ganong-Levine syndrome (LGL) is the other important pre-excitation syndrome. It occurs due to the presence of James fibres, accessory conducting fibres that connect the atria (or the beginning of the AV node) to the bundle of His. These fibres bypass the AV node completely or partially.
These fibres don’t allow one ventricle to be depolarized before the other; the ventricles are depolarized normally via the His and Purkinje fibres. There are no delta waves, and the QRS is normal.
Like in WPW, these patients experience episodes of paroxysmal supraventricular tachycardia due to AVRT.
ECG morphology:
- Short PQ-interval
- Delta waves absent
- Normal QRS complexes
Recent studies have called into question whether all patients with LGL syndrome have James fibres. Some may simply have “enhanced atrioventricular nodal conduction” instead.
Hey Greek,
Just wanted to point out the typo LPL, which is suppose to be LGL
Have an awesome day!
Fixed,
Cheers
It’s also mentioned in the very last paragraph, but now I’m being picky(!) and unsure whether the corrections are helpful or not.
Thanks for everything!