Table of Contents
Page created on December 17, 2018. Last updated on December 18, 2024 at 16:56
Respiratory acidosis
Definition
In respiratory acidosis we have:
- pH below 7.35
- Increased pCO2
- Increased actual bicarbonate
When kidney compensation kicks in, after around 24 hours, will we also have:
- Increased standard bicarbonate
- Increased buffer base
- Positive base excess
Etiology
Because it is respiratory, it’s caused by a primary increase in pCO2, due to inadequate ventilation. This decreases the pH. When pCO2 increases will actual HCO3– also increase because they’re in an equilibrium. We’ll get to the compensation later.
Recall that CO2 diffuses really easily in contrast to O2, so diffusion disorders rarely lead to elevated pCO2. Only hypoventilation will.
The only cause of respiratory acidosis is alveolar hypoventilation, which causes global respiratory failure,. We’ll repeat some causes here.
Common causes include:
- Airway obstruction
- Asthma
- COPD
- Obstructive sleep apnoea syndrome
- CNS disturbances
- Central sleep apnoea
- Accidents
- Tumors
- CNS depressant drugs
- Morphine
- Sedatives
- Cardiac and pulmonary
- Pulmonary oedema
- Pulmonary embolism
- Pulmonary fibrosis
- Restrictive lung diseases
- Respiratory muscle weakness
Not all of these warrant an explanation, but some of them do.
CNS disturbances damage or depress the respiratory centre, which decreases the respiratory drive. Morphine is especially known for depressing the respiratory centre.
Consequences
- Hypercapnia causes brain vasodilation, which can increase the intracranial pressure
- Chronic hypercapnia is well tolerated, but it causes the respiratory centre to be less sensitive to CO2, potentially causing breathing to be driven by hypoxia instead
- If the acidosis is severe the consequences will be similar as for metabolic acidosis.
Compensation
Intracellular buffers start working after 6 – 8 hours. However, they aren’t very effective. There will only be 1 mmol/L increase in serum bicarbonate for every 10 mmHg increase in pCO2.
Because kidney compensation doesn’t kick in until after 24 hours can we distinguish two phases of respiratory acidosis, the acute phase and the chronic phase. In the chronic phase as the kidney started to retain more bicarbonate, in order to increase the bicarbonate:CO2 ratio toward the normal 20:1.
When the kidney starts to retain bicarbonate will the standard bicarbonate also rise. In this phase will there be a 4 mmol/L increase in serum bicarbonate for every 10 mmHg pCO2 increase, which is 4 times more efficient than in the acute phase.
The parameters change like this:
| Parameter | Acute phase (no compensation) | Chronic phase (yes compensation) |
| pH | Decreased | Decreased less or normal |
| pCO2 | Increased | Increased |
| Actual HCO3– | Increased | More increased |
| Standard HCO3– | Normal | Increased |
| Buffer base | Normal | Increased |
| Base excess | 0 | Positive |
Treatment
Artificial ventilation may be used to wash out excess CO2. The underlying cause should be treated.
Respiratory alkalosis
Definition
In respiratory alkalosis we have:
- pH above 7.45
- Decreased pCO2
- Decreased actual bicarbonate
When kidney compensation kicks in, after around 24 hours, will we also have:
- Decreased standard bicarbonate
- Decreased buffer base
- Negative base excess
It’s basically the opposite of respiratory acidosis.
Etiology
The only way to have too low pCO2 is by alveolar hyperventilation, the causes of which have already been discussed. Here are the most important:
- High altitude
- Anxiety
- Pain
- Pregnancy
- Hypoxaemia
Hypoxaemia causes hyperventilation as a compensatory reaction. If the arterial pO2 falls below 60 mmHg the hypoxaemia start to stimulate ventilation.
Consequences
- Hypocapnia causes cerebral vasoconstriction, reducing the cerebral blood flow which can cause hypoperfusion, leading to unconsciousness and syncope
- Alkalosis causes:
- Decrease in ionized Ca2+, just like in metabolic alkalosis. Neuromuscular excitability increases, potentially causing tetany, laryngospasm, and suffocation
- → Extracellular K+ concentration decreases → hypokalaemia -> risk for arrhythmia increases
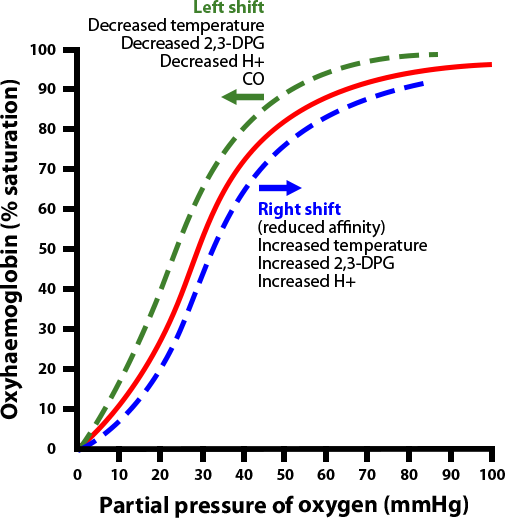
- Haemoglobin-oxygen dissociation curve is shifted to the left, which decreases tissue oxygenation.
- In severe cases similar symptoms to metabolic alkalosis may occur.
When the blood becomes more alkaline will albumin become more ionized to its negative form. This causes it to bind more Ca2+, which reduces the ratio between ionized (free) Ca2+ and bound calcium in the blood. Only ionized calcium is physiologically active, so the active amount of calcium in the blood is effectively reduced. Calcium blocks sodium channels and inhibits depolarization. When calcium levels are reduced will the threshold for depolarization be lowered. This causes increased neuromuscular excitability, which can cause tetany that might affect the larynx, which can cause suffocation and death.
Alkalosis causes hypokalaemia by moving potassium out of the plasma and interstitial fluids into the urine. This is caused by the effects of intercalated cells in the collecting duct. The kidney wants to conserve H+ ions, but to do so it must excrete K+ ions to maintain electroneutrality. Hypokalaemia is arrhythmogenic through several mechanisms. Hypokalaemia makes the membrane potential more negative, making it harder to reach the threshold for depolarization.
Lastly will the alkalosis cause a left-shift of the oxygen-haemoglobin dissociation curve, meaning that oxygen now binds more strongly to haemoglobin. This causes the amount of oxygen released from haemoglobin into the tissues to be decreased.
Compensation
The situation is similar as for respiratory alkalosis. In the acute phase will only intracellular buffers work, but in the chronic phase will the kidneys excrete more bicarbonate.
In the acute phase will there be a cause a 2 mmol/L decrease in HCO3– for every 10 mmHg decrease in pCO2.
In the chronic phase will there be a cause a 4 – 5 mmol/L decrease in HCO3– for every 10 mmHg decrease in pCO2.
The parameters change like this:
| Parameter | Acute phase (no compensation) | Chronic phase (yes compensation) |
| pH | Increased | Increased less or normal |
| pCO2 | Decreased | Decreased |
| Actual HCO3– | Decreased | More decreased |
| Standard HCO3– | Normal | Decreased |
| Buffer base | Normal | Decreased |
| Base excess | 0 | Negative |
Treatment
Treatment involves treating the underlying disorder. If caused by anxiety, breathing into a bag can also help.
If there is significant hypocalcaemia calcium may be administered.
Mixed acid-base disorders
What happens if there are multiple conditions present in the same person, where one would cause an alkalosis and the other an acidosis? The answer is that they could cancel each other out to some degree. pH may even become normal. That doesn’t mean that everything is fine – other components of the conditions could be dangerous.
We can also have respiratory alkalosis and metabolic alkalosis at the same time, where they worsen each other. The same goes for acidosis.
Some examples where there could be a mixed acid-base disorder:
Heart failure patient with pulmonary oedema. The patient may develop lactic acidosis because of hypoxaemia, and respiratory alkalosis or acidosis because of pulmonary oedema.
ICU patients with artificial ventilation and nasogastric suction. Respiratory alkalosis + metabolic alkalosis can occur.
Liver failure patient with ascites. The fluid loss into the abdomen causes secondary hyperaldosteronism. Liver failure causes type B lactic acidosis, and hyperaldosteronism causes metabolic alkalosis.
Hi! Under the consequences of respiratory alkalosis you write that extracellular K+ is decreased leading to hyperkalemia, but in the section beneath you write that it is hypokalemia, and that leads to arrythmia?
Just a small typo, hypokalaemia is correct. Corrected now.
Also, if you leave comments in the future, leave the e-mail field blank. Including an e-mail makes the comment marked as spam, and so I might miss them.
Pulmonary edema by itself it leads to respiratory acidosis, but it is frequently treated with diuretics, causing metabolic alkalosis. But still I don’t know if pulmonary edema can lead to alkalosis without diuretics…