Table of Contents
Page created on September 29, 2018. Last updated on December 18, 2024 at 16:56
A cardiomyopathy is a disease of the myocardium which is not caused by coronary artery disease, hypertension, valvular disease or congenital heart diseases. In other words, myocardial diseases caused by hypertension, coronary artery disease, valvular disease or congenital heart diseases are not considered cardiomyopathies.
Some definitions include the aforementioned diseases as cardiomyopathies, but most definitions don’t. Source
Cardiomyopathies are either primary or secondary. Primary cardiomyopathies are caused by diseases that only or prediminantly affect the myocardium. Idiopathic or genetic causes are usually in the background. Secondary cardiomypathies are caused by myocardial involvement in systemic diseases.
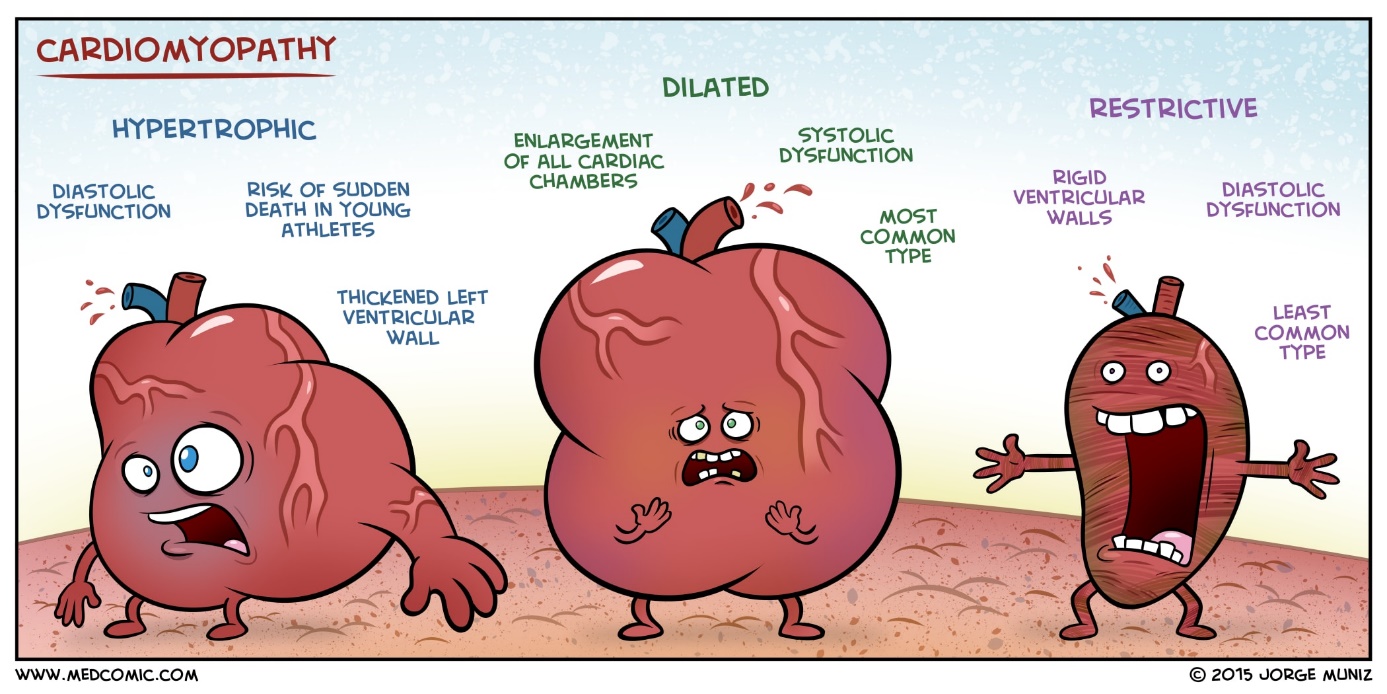
We distinguish four types of cardiomyopathy: Dilatative, hypertrophic, restrictive and arrhythmogenic right ventricular cardiomyopathy. Each of them can have two types of causes: primary and secondary.
Dilatative cardiomyopathy
Dilatative cardiomyopathy is the most common cardiomyopathy. It’s characterised by dilation and impaired contraction of one or both ventricles. In dilatative cardiomyopathy the ventricular wall is continuously thinning, which increases the lumen of the ventricle. It leads to a decrease in ejection fraction with a decreased cardiac output, eventually causing heart failure.
It’s primary in 50% of cases, which is idiopathic. There are probably some genetic components.
Secondary causes of dilatative cardiomyopathy:
- Pregnancy
- Beri beri (Thiamine deficiency)
- Coxsackie B myocarditis
- Alcohol abuse
- Cocaine abuse
- Rheumatic heart disease
- SLE
Hypertrophic cardiomyopathy
In hypertrophic cardiomyopathy the ventricles (mostly the left) are abnormally hypertrophic. The primary type is more common than the secondary type. There are two types:
- Non-obstructive type – where the septum is not hypertrophic
- Obstructive type – where the septum is hypertrophic
In the obstructive type the septum can be so hypertrophic that it obstructs the outflow tract of the left ventricle, completely ceasing cardiac output. This is a common cause of sudden cardiac death in young people.
In both types the hypertrophic ventricle has reduced compliance, so a high EDp is required to fill it. The contraction force is high, yielding an ejection fraction of almost 100%! The obstructive type is the worst of the two.
Primary hypertrophic cardiomyopathy is caused by mutations in the genes for the myosin heavy chain. It follows an autosomal dominant inheritance pattern.
Secondary hypertrophic cardiomyopathy has the following causes:
- Friedreich’s Ataxia
- Pompe’s disease
Restrictive cardiomyopathy
Restrictive cardiomyopathy is very rare. Something causes proliferation of connective tissue in the myocardium, which causes the ventricular wall to become restrictive and lose compliance. When the walls are stiff the EDp must be high to fill the ventricle, which causes backward venous congestion.
It’s mostly caused by secondary causes like:
- Amyloidosis
- Sarcoidosis
- Hemochromatosis
Arrhythmogenic right ventricular cardiomyopathy
This is another rare type of cardiomyopathy. It’s characterized by a fatty or fibrotic degeneration of the right ventricle, causing the ventricular wall to become thinner and the ventricle itself to become dilated. As the name implies arrhythmias often occur.
It can cause sudden cardiac death in healthy young people due to lethal arrhythmias.
Only primary, idiopathic causes are known.
hi.
can you please explain why high EDp is needed in caase of reduced compliance in hypertrophic ccardiomyopathy?
thanks in advance.
When the ventricles have reduced complience, more pressure is needed to fill them. As such, the end-diastolic pressure must increase to keep filling the ventricles.
thank.
welc.