Table of Contents
Page created on October 22, 2018. Last updated on December 18, 2024 at 16:56
Breathing mechanics
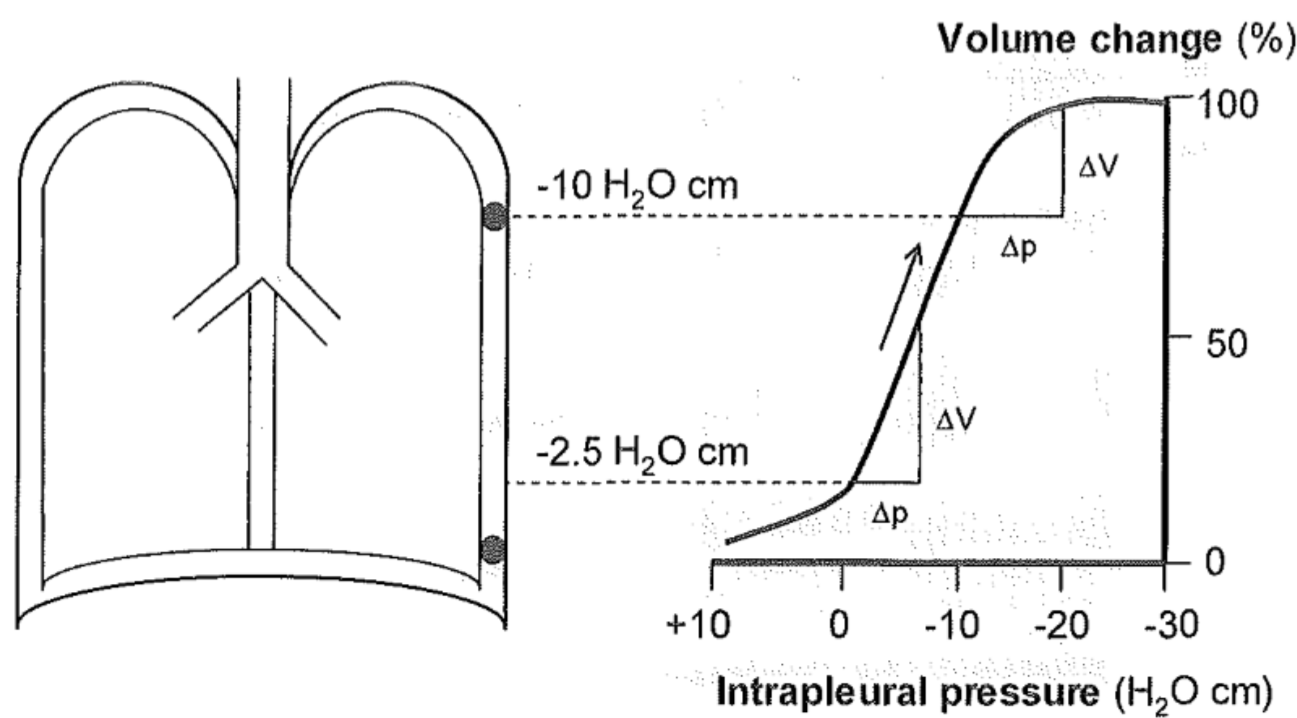
The pressure in the pleural space, the space between the visceral and parietal layers of the pleura is -4 cmH2O in rest. The intrapleural pressure is -10 cmH2O in the apex of the lung and -2.5 cmH2O in the base of the lung. In other words, the intrapleural pressure is higher at the level of the base than at the level of the apex. This is due to gravity pulling the air down to the base from the apex.
To breathe in the thoracic cavity must expand. When the intercostal muscles contract the chest expands. When the diameter of the thorax increases by 1 cm due to this will 200 mL of air enter the lungs. The thoracic cavity is also enlarged when the diaphragm contracts, which pushes down the abdominal organs. When the diaphragm is lowered 1 cm will 350 mL of air enter the lungs. The take home message is that the diaphragm contributes more to the inflow of air then the intercostal muscles.
When the respiratory muscles contract the thoracic cavity will expand. The negative intrapleural pressure causes the two layers of the pleura to “stick together”. When the parietal pleura expands with the chest the negative intrapleural pressure causes the visceral pleura to be pulled with it. Because the visceral pleura is attached to the lungs the lungs will expand as well, causing air to fill the lungs.
While inspiration is an active process (muscles contract) is expiration during rest a passive process (no muscle work is needed). During inspiration the elastic fibres in the lung are stretched, and when the respiratory muscles relax these stretched fibres will compress the lung, like a rubber band that is released. When the lungs are compressed the lungs will press on the air inside, which will cause the alveolar pressure to increase above atmospheric pressure, which causes air to exit through the only openings available, the mouth and/or nose.
Compliance is the measure of how easily something can stretch. If you have an old rubber band it will stretch quite easily, but if you buy a new one, you’ll probably see that it’s harder to stretch. The old rubber band has higher compliance.
The normal compliance of the lung is above 2 litre/kPa, meaning that when the pressure changes by 1 kilopascal 2 litres of air will flow into or out of the lung. When lung compliance is low it becomes much harder to fill the lungs with air. However, a too high compliance (as seen in disease) isn’t good either, as we’ll see later.
Elastic resistance
Because the intrapleural pressure is higher at the level of the base than the apex will the alveoli at the base will be subject to more pressure than the alveoli at the apex after expiration. This causes alveoli on the base to be more compressed and therefore contain less air than apical alveoli, after expiration.
When air flows through the trachea and fills up the alveoli, the alveoli that require the least work to fill will be filled first. Because the apical alveoli are already slightly filled with air compared to the basal alveoli, more work is required to fill them further. Because it is easier to fill the basal alveoli than the apical alveoli, the basal alveoli have higher compliance. In other words, the compliance is higher in the alveoli in the base of the lung than in the alveoli in the apex of the lung.
The result of this is that ventilation, the amount of air moving in and out of the alveoli, is higher in the base than in the apex. This will become important in topic 46.
The higher the compliance the lower the elastic resistance.
Non-elastic resistance
When breathing in we don’t just have to overcome the elastic resistance, but other resistances as well. The non-elastic resistance is the sum of the airway resistance and the viscous resistance of the tissues.
The airway resistance (Raw) depends mostly on how easily the air flows in and out of the airways. The normal value of airway resistance is less than 0.3 kPa/litre/second. In other words, less than 0.3 kPa of pressure is needed to produce an air flow of 1 litre per second.
Recall from biophysics the concept of fluid mechanics. A fluid (or a gas) can flow in a tube in a nice, clean and organized way, called laminar flow, or in a messy, disorganized way, called turbulent flow.
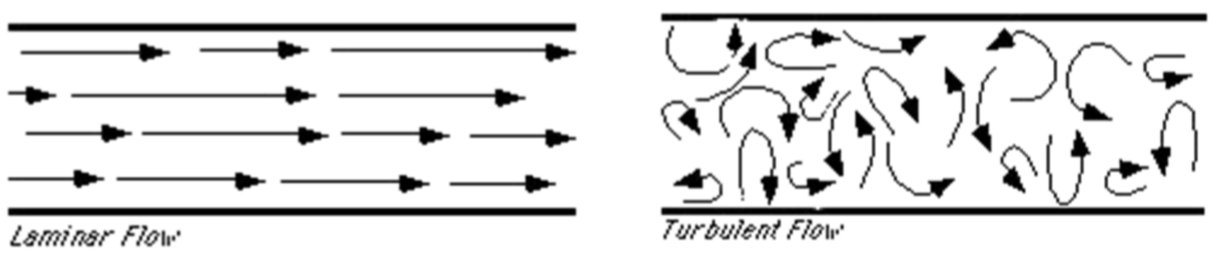
Air flows the easiest when the flow is laminar. Several things can cause turbulent air flow, like tachypnoea (too fast breathing), abnormal dimensions of the airways and the viscosity of the air as well.
The work of breathing
The work of breathing can be thought of the energy of breathing, or how difficult it is to breathe (work is here used as the same sense as in biophysics). The work of breathing is defined as the work used to overcome the elastic resistance plus the work used to overcome the non-elastic resistance. Because exhaling is a passive process is work not required for exhaling, only for inhaling.
It’s important to find a combination of breathing frequency and breathing deepness that is efficient. The elastic resistance increases when the lung volume increases, so taking super-deep breaths requires a lot of work. At the same time, breathing very fast and often causes turbulent air flow and therefore raises the airway resistance. The logical conclusion is that the optimal breathing pattern is not too fast and not too slow, and not too deep and not too shallow but rather somewhere in between.
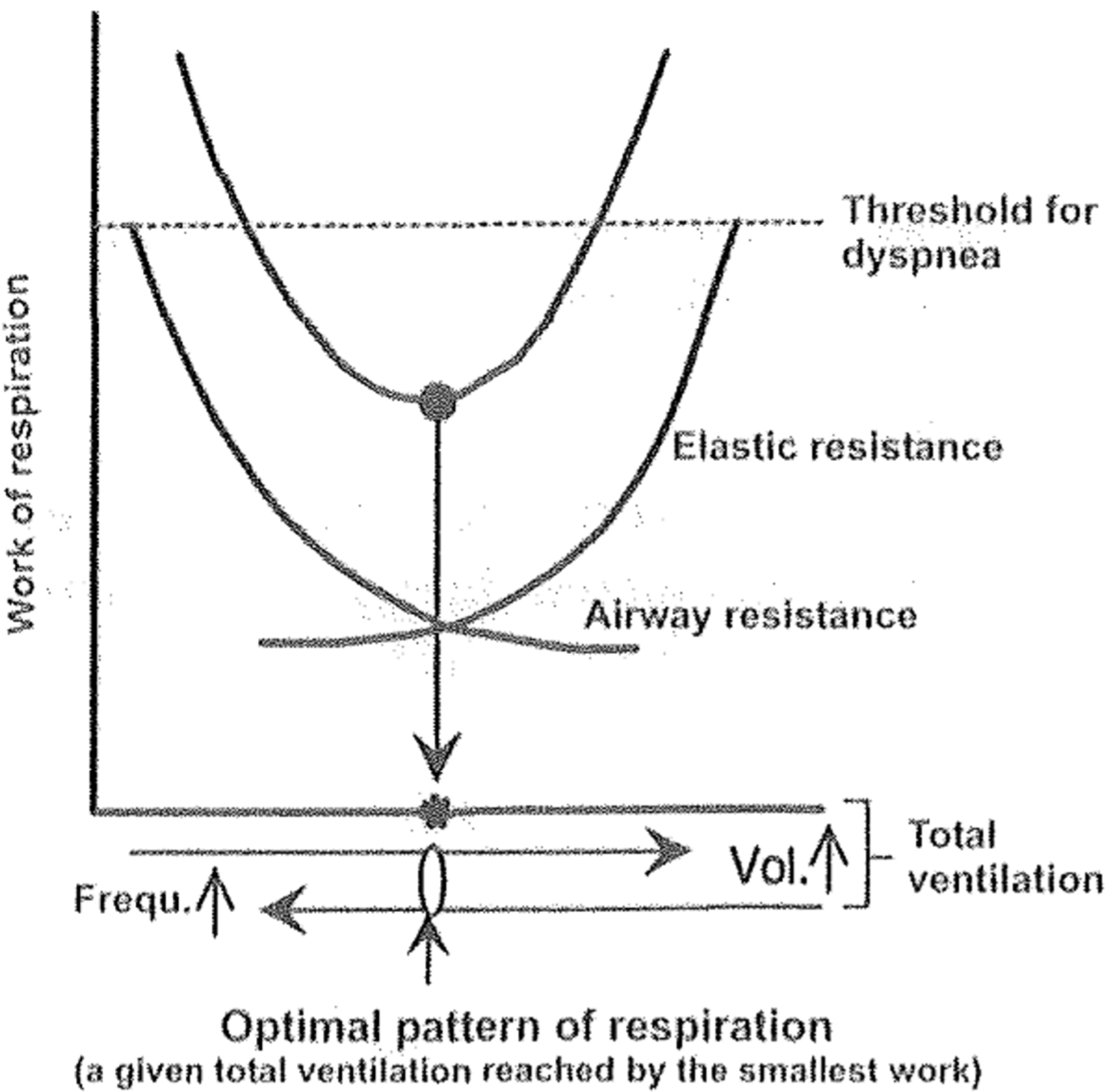
On the figure above we can see exactly that. When we increase the volume of each breath too much (going too much to the right on the x-axis), the work of breathing increases. Also, when we increase the breathing frequency too much (going too much to the left) the work of breathing also increases. The ideal respiration pattern is where the work of breathing is lowest (the lowest point of the U). The normal, most efficient respiratory pattern is when we take a breath approximately 14 times per minute and each breath is approximately 500 mL deep.
The respiratory muscles need oxygen as well. In physiological conditions, when the work of breathing is kept to a minimum is this amount very low. The average oxygen consumption needed for respiration in rest is about 1 mL O2 per 1 L of air ventilated. That’s approximately 8 mL of O2 per minute for the process of respiration, which is just 2-3% of the total oxygen consumption of the body.
The work of breathing is increased in:
- Tachypnoea
- Emphysema
- Obesity
- Congestive heart disease
Disorders causing abnormal compliance
Restrictive lung disorders is characterised by decreased compliance.
There is one disorder where the compliance is abnormally increased. In the case of emphysema are the septa between the alveoli destroyed. This causes the compliance to increase a lot. This makes it very easy for the lung to fill up with air, however the passive recoil of the lung is mostly lost, meaning that the lung can’t be sufficiently emptied of air! As a consequence will the residual volume of the lung increase. The emphysemic patient will have no problem with inhaling but will struggle to exhale! Because the patient can’t renew all the air in the lung can respiratory failure soon develop. You can read more about emphysema in topic 50.
Hi Nikolas,
I find in the textbook of pathophysiology, the intrapleural pressure is about -4 cmH2O during respiration , but you mentioned is in rest.
The pressure seems to be the same throughout the breathing cycle, according to these two sources:
https://open.oregonstate.education/aandp/chapter/22-3-the-process-of-breathing/
https://www.ncbi.nlm.nih.gov/books/NBK559004/
In either case, the exact value of the pressure is not important.