So I had pharma 3 yesterday. My examiner was prof. Gábor Pozsgai and he was very nice. I got two topics I liked and one which was meh, but I was hoping to get the 5 this time. In the end he asked me many things I couldn’t answer, and so I got a deserved 4.
There were four examiners who examined yesterday. Prof. Pozsgai, prof. Pethő, prof. Barthó and dr. Bölcskei. Prof. Helyes and prof. Pintér were not present.
You draw three topics, one from each pharma semester. My topics were “Local anaesthetics”, “Laxatives, antidiarrhoeal agents, drug treatment of inflammatory bowel disease and paralytic ileus, digestives, drugs used in cholelithiasis” and “Antiviral drugs against herpes, hepatitis and influenza viruses”.
As you might notice, my pharma 3 topic included influenza viruses, which, according to the topic list in the course information, should belong to the HIV topic. They moved influenza drugs from the HIV topic to the herpes and hepatitis topic.
Drug walk
My first question was to define potency. I defined potency correctly, but when I messed up when defining the ED50. I said that the ED50 is the concentration which gives the desired effect in 50% of patients, which is wrong. He told me that it was wrong, I corrected it and it was fine.
Then he asked me the differences between first and second generation antihistamines. I said that the first generation ones penetrate the BBB more easily, causing more sedation, and that the first generation ones block muscarinic receptors to a larger degree, causing side effects like dry mouth and constipation.
Then he asked me which drugs could be used in congestive heart failure. I said ACE inhibitors, AT2 antagonists, beta blockers, calcium channel sensitizers, cardiac glycosides and diuretics. He asked me what the indications for cardiac glycosides would be, as they’re not first-line agents. I didn’t know, but he said that they’re used if the patient has another condition in addition to the heart failure. I remembered that glycosides are anti-arrhythmics (even though I forgot to include them in the anti-arrhythmic topic, whoops), and so I said that maybe they would be preferred if there was also an arrhythmia. He said yes and asked which arrhythmia. With a qualified guess I said atrial fibrillation, which was correct.
Then he asked me to list the types of antianxiety and hypnotic drugs. I mentioned benzo’s, barbiturates and z-drugs. He asked me for a drug which is an anxiolytic but has no hypnotic effect. I asked if he meant any antidepressants, but that’s not what he was after. I remember that there were some atypical anxiolytics mentioned at the end of the benzo topic, but I couldn’t remember the name or the mechanism. He helped me by saying that it acts in a different manner than the other anxiolytics, but in the end I couldn’t produce the answer. He said that he was after buspirone. To be honest I had that name in my head when I was trying to find the answer, but I wasn’t sure so I never said it. Just goes to show that you should trust your gut.
He then asked me about the types of oral antidiabetics which don’t carry a risk for hypoglycaemia. I said metformin, GLP-1 agonists, DPP-4 inhibitors, SGLT-2 inhibitors and glitazones (I forgot the alpha-glucosidase inhibitors). He asked me which ones increase the risk for urinary tract infections, and I said the SGLT-2 inhibs. He asked me if I could name any, but I was honest with him and told him that I have given up trying to remember the names of the oral antidiabetics. It was fine, and we moved on to topics. He asked me which topic I wanted to start with.
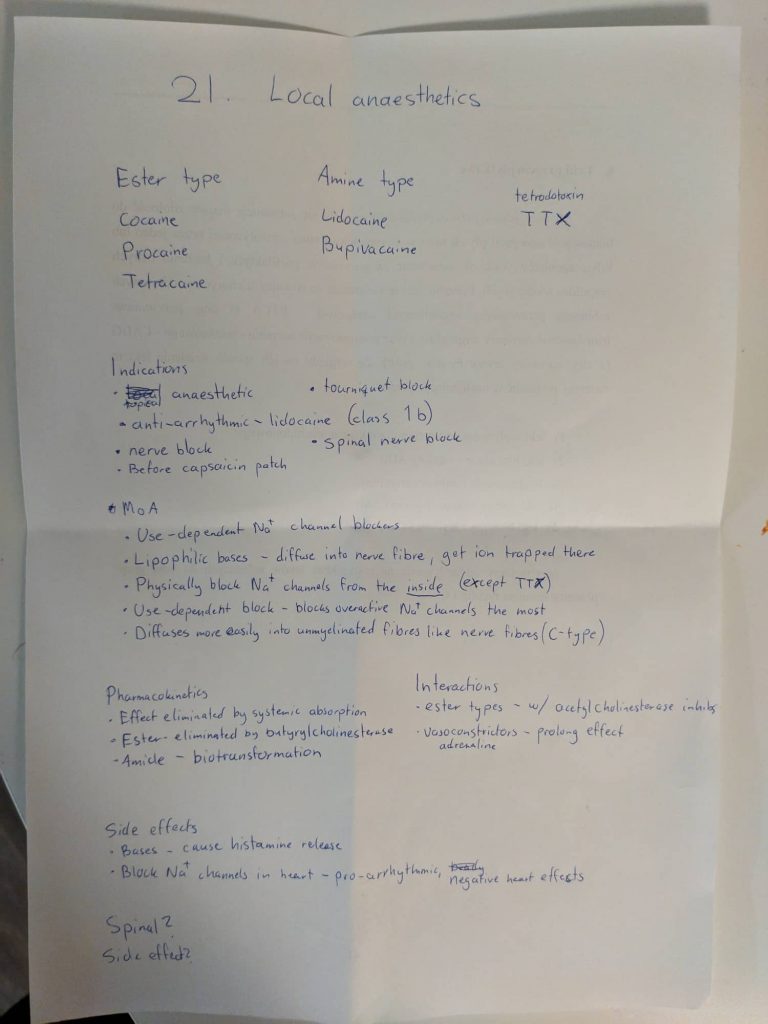
Local anaesthetics
I didn’t present the topic, he started by asking questions.
- Examiner: What is the mechanism of action of local anaesthetics?
- Me: They block sodium channels from the inside of the cell. They must diffuse into the cell, so they’re lipophilic. Inside the cell they’re ion-trapped, because these drugs are bases. This block is use-dependent.
- E: What does it mean that it’s use-dependent?
- M: It means that these drugs preferentially block the more active sodium channels.
- E: What are the mechanisms behind this?
- M: The drugs physically block the opening of the channels, so the more often the channels are open the more opportunities the drug has to plug it.
- E: Yes, and there’s one more mechanism.
- (I didn’t know that)
- E: It has to do with its conformation.
- M: Do they stabilize the channels in their inactive conformation?
- E: No, not really.
- M: Then I don’t know.
- E: Okay, what can you say about the pharmacokinetics of these drugs?
- M: Their effect is terminated when they’re absorbed into the systemic circulation.
- E: Yes. Can you mention some side effects?
- M: Yes, they’re bases so they can cause histamine release (I don’t know if this is true actually). They’re also cardiotoxic, so they can cause arrhythmia and negative heart effects.
- E: Not really arrhythmias, but negative heart effects, yes. There are some special side effects when they’re given as spinal anaesthesia.
- M: I don’t know.
- E: They’re really characteristic side effects.
- M: I don’t know.
- E: Okay. Can you mention some local anaesthetics?
- M: Yeah (I listed the ones I had written down).
- E: Which is more long-acting, tetracaine or procaine?
- M: Tetracaine. (Pure guess)
- E: Yes. Do you know anything special about bupivacaine?
- M: Hmm, I remembered prof. Gregus talked about the treatment of its intoxication.
- E: Yes, what was that?
- M: So bupivacaine is cardiotoxic, and if it’s injected into a vessel by accident it can be fatal. It’s lipophilic. By giving a lipid formulation like intralipid intravenously the lipid formulation can “dissolve” bupivacaine out of the heart.
- E: Yes, do you know the original use of intralipid?
- M: Yes, it’s used for parenteral feeding.
- E: Yes, next topic.
Laxatives, antidiarrhoeal agents, drug treatment of inflammatory bowel disease and paralytic ileus, digestives, drugs used in cholelithiasis
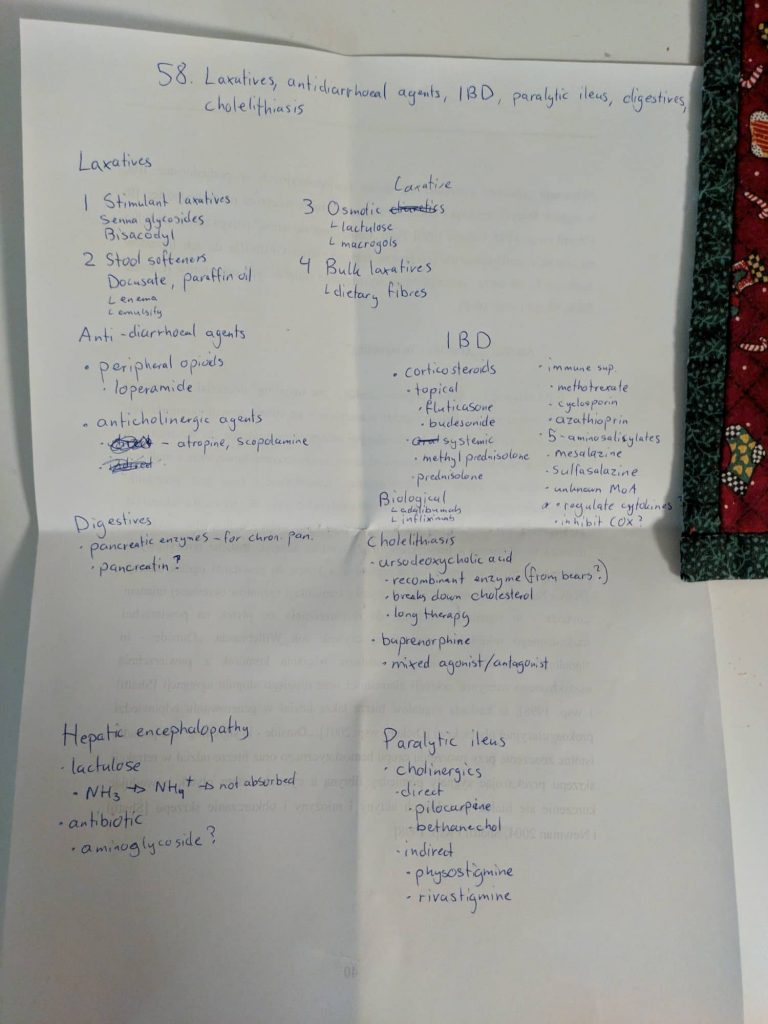
- M: Okay, so we have four types of laxatives. Bulk laxatives, osmotic laxatives, faecal softeners and stimulant laxatives.
- We talked a bit about laxatives, I don’t remember exactly what was said. I remember some of his questions
- E: What’s another use for lactulose?
- M: It’s used to treat hepatic encephalopathy.
- E: And how does that work?
- M: It acidifies the lumen of the GI tract, protonating ammonia to ammonium, preventing it from being absorbed.
I forgot the non-absorbable salts as osmotic laxatives. He tried to make me remember them by giving me some hints, but I had forgotten that they existed. He also talked about a faecal softener which is not on greek doctor and which I had never heard about. He also asked about the pharmacokinetics of senna glycosides, which I knew nothing about. Do they even have any pharmacokinetics? I also forgot adsorbents as antidiarrhoeal agents, and mebeverine.
- E: Can you give me the drugs used to treat IBD? (funny, I was asked the same thing in pharma 2, and I have Crohn’s, so. Ironic)
- I listed the ones I had written down, but while reading them I realized that I had forgotten to write down the biological treatment, but I remembed their name.
- E: Which disease is the biological drugs more important in?
- M: Crohn’s. (I’m actually going to start adalimumab in a few weeks)
- He didn’t ask me anything else in this topic.
Antiviral drugs against herpes, hepatitis and influenza viruses
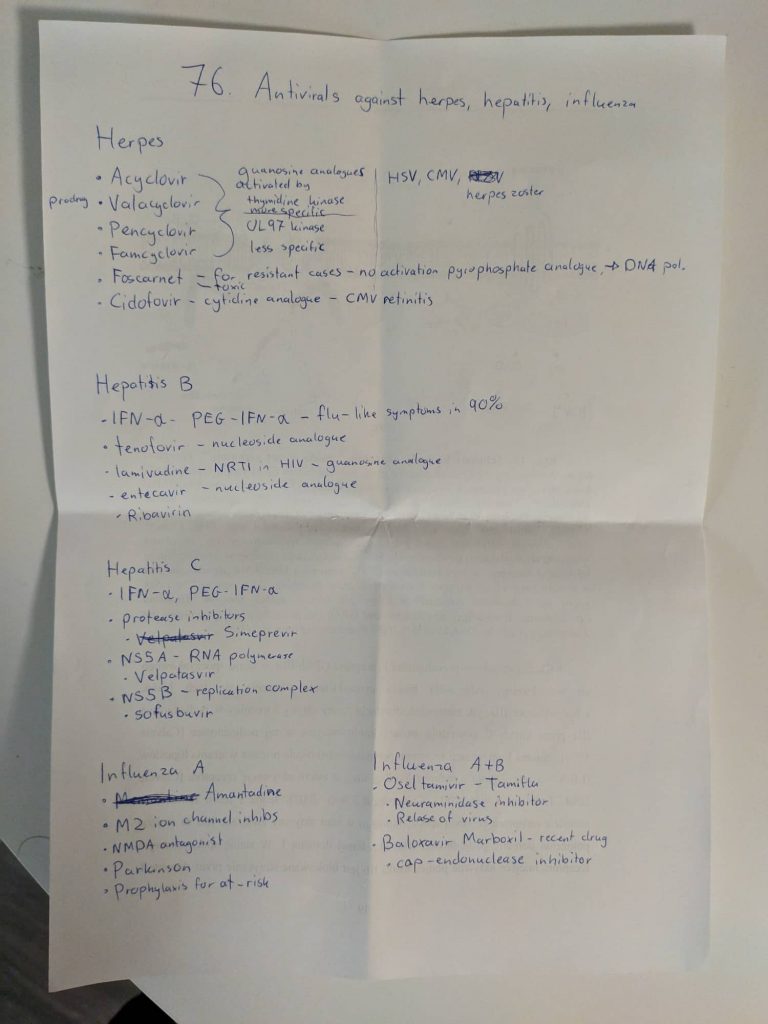
I began by listing drugs against herpes viruses. He asked about the mechanism of action of foscarnet. He asked me why we need prodrugs for these antivirals. Then he asked me about antivirals to treat EBV, or so I heard. I’m pretty sure I heard EBV, but I might have heard wrong, or he might have said wrong, because I’m pretty sure he was after ganciclovir and valganciclovir, which are used to treat CMV, not EBV. He asked me how antivirals are specific against virally infected cells.
- E: What are the side effects of these drugs?
- M: CNS toxicity? Hepatotoxicity?
- E: No.
- M: Nephrotoxicity?
- E: Yes. How are these antivirals metabolized?
- (I was pretty sure that they’re not metabolized but rather excreted renally unchanged. But I also didn’t think that he’d ask me a trick question like that, so I started guessing)
- M: Are they metabolized by xanthine oxidase?
- E: No, they don’t resemble nucleosides enough for that.
- M: Then I don’t know.
- E: They’re not metabolized, they’re excreted renally.
- M: (jesus) So it was a trick question?
- E: Yes (said with a stone cold face)
Then we went on to the hepatitis B drugs. He started by asking which hepatitises can be treated pharmacologically. I said B and C. I then listed the drugs I had written down.
- E: What is the other use of these drugs?
- M: Against HIV.
- E: Yes. What’s different in the treatment of hep B and C?
- M: The treatment of acute hepatitis C is curative.
- E: Yes.
We went on to hepatitis C. I listed the drugs.
- E: There is another drug which is very old, but still used. It might’ve been mentioned in other topics but it’s also used to treat hep C.
- M: I don’t really know.
- E: It causes some haematological side effects.
- M: Ribavirin?
- E: Yes.
He might have asked me some other questions about hep B and C, but I can’t remember now. We went on to influenza drugs.
- M: Amantidine is used in influenza A. It inhibits an ion channel called M2, which is important for viral replication.
- E: Can you be more precise about the step in the replication the M2 channel is important for?
- M: No, not really. I don’t know.
- E: Okay, continue.
- M: We have oseltamivir, used for both influenza A and B. It inhibits neuraminidase, which is necessary for the release of the virus out of the cell.
- E: Yes.
- M: There is also baloxavir marboxil, which inhibits cap-endonuclease or something.
- E: I’ve never heard of this drug.
- M: Oh, haha. It was talked about in the seminar. It’s very recent I think.
- E: Okay. There is a drug which has similar action to oseltamivir but has a very special way of administration.
- M: Oh yeah. It starts with z, I don’t remember the name. It’s given by inhalation
- E: I wouldn’t really say that it’s inhaled.
- M: What? Then I don’t know.
- E: It’s given by nasal spray.
It doesn’t say that on the seminar or in the book. It says that it’s given as a powder for oral inhalation, so he was definitely wrong about that.
And that was that. He spent a long time examining (especially compared to other examiners), but he was very nice.
Next
I have haematology on thursday and clinical biochem on monday.
I think greek.doctor is nearing its end. There aren’t any more subjects I want to write notes for, and I’m very, very tired of doing this. It takes a lot of time and energy, maybe more than most people think. Right now there are 817 pages, only maybe 10 of which aren’t topics and the vast majority of which I’ve written myself (the rest are written by my girlfriend, Sofia (msworldwide)). Almost all of these 817 pages are multiple pages long documents, and I spend maybe 2-3 hours per topic on average. I’ve been giving myself a lot of work by doing this, and I’m very glad that I did (maybe except for hema), but now I need time for myself to work on my mental health and engage in my hobbies.
I won’t take down the website. I’ll keep it up until it’s no longer used, which could be never. I’ll continue to maintain it by answering comments and fixing errors. I’ll post some statistics at the end of the exam period, as people seem to like that, and I think we’ll break the record again (like we do every exam period).
Oh, and by the way, I’ve made less than 5 euro from the advertisement on the page. I’ll keep it until the end of the exam period, but I’ll probably remove it as it’s not really worth having.
“asked me how antivirals are specific against virally infected cells.” Can you please explain why they are specific ?
Because they’re activated by kinases only found in virally infected cells.
Is there anything we can do to help you make money on the ads? Do we just click them?
I get more revenue with clicks than views, yes, but please don’t click if you’re not interested. Don’t do it for the revenue’s sake.
you rock, don’t ever change.
<3
Congrats on the exam!! and bless you for not taking the website down! but i was wondering even if you don’t write any more notes for your future subjects, could you still do the exam experiences? i think its really helpfull with some insight for future semesters :))
Thank you!
Sure, I don’t mind doing that. I didn’t know people found them helpful.
Congrats! Also thank you for not taking the website down! Good luck with the rest of your exams.
Thank you, same to you!
Mental health is real