Table of Contents
Page created on March 19, 2018. Last updated on December 18, 2024 at 16:56
Introduction
The normal pH value of the blood is 7.35 to 7.45. Below it is acidosis, and above alkalosis. The pH range that is compatible with life however is 7.0 to 7.9. The stomach lumen has a pH of 1.5 to 2, while the mucosal lining of the stomach has pH 7. Lysosomes and endosomes in the cell are pH 5 while mitochondria are pH 8. [HCO3–] in the blood is normally 24 mM while pCO2 is 40 Hgmm.
The pH buffer in the blood, comprised of HCO3– and dissolved CO2, constantly works to keep the pH in the normal range. Several processes both produce and remove acids. Most of the acid comes from produced CO2, but also from lactic acid, ketone bodies and other organic acids. Acid is removed through respiration, by secretion through the kidneys and also by metabolism, when an acid is involved in a metabolic process that neutralizes the acid, like in Cori cycle.
Several processes in the body produces HCO3– and NH4+. They’re both excreted by the kidney as urea. CO2 is produced by pyruvate, α-ketoglutarate and branched-chain α-keto acid dehydrogenase complexes and in the pentose phosphate pathway, among others. CO2 is consumed in carboxylation reactions.
CO2 produced by tissues will diffuse into red blood cells, where carbonic anhydrase will convert it into HCO3–. When the blood reaches the lungs, the reaction will run the opposite way to produce CO2, which will diffuse through the blood-air barrier to be excreted.
The body must control the CO2 / HCO3– equilibrium to keep the blood pH in the normal range. Chemoreceptor cells in the medulla oblongata can sense the concentration of CO2 in the blood and adjust the equilibrium accordingly by increasing or decreasing respiration.
Lactate
Lactate is produced during anaerobic breakdown of glucose, like in hypoxia, RBC or during heavy muscle work. It is also produced in aerobic conditions when the glycolysis produces pyruvate faster than the mitochondria can degrade the pyruvate, which happens in fibroblasts, thrombocytes, lymphocytes, brain and the kidney medulla.
Lactate is transported to the liver (mostly) and kidney cortex to be converted to glucose through gluconeogenesis.
Lactate overproduction can cause lactic acidosis and can be a result of intense muscle work or oxygen supply problems, like anemia or cyanide toxicity.
Decreased lactate removal will also cause lactic acidosis. Liver insufficiency, due to alcohol or certain enzyme defects, will lower the livers ability to convert lactate to pyruvate. High ingestion of fructose will cause overproduction of pyruvate, because F-1-P and F-1,6-BP activate pyruvate kinase, and fructose breakdown skips PFK-1, which is the main regulator of glucose degradation.
When the activity of pyruvate dehydrogenase complex reached 15-30% of normal, there will also be lactic acidosis. This can be caused by thiamine deficiency or as an inborn enzyme defect.
Lastly, pyruvate carboxylase deficiency will also cause lactic acidosis while also disturbing other processes, like neurotransmitter synthesis, urea cycle and others.
Ketone bodies
Ketone bodies are formed after the body has run out of glycogen and glucogenic amino acids. The body will start to break down triacylglycerols into glycerol and free fatty acids. The body will use available oxaloacetate to feed the gluconeogenesis. Because OAA is also an intermediate in the TCA cycle, the cycle will slow down. This causes acetyl-CoA to accumulate, which will be converted into ketone bodies.
Ketone bodies are acidic, so they will reduce the blood pH. However, normal, healthy people won’t be negatively affected by this, as their bodies can compensate for the presence of these ketone bodies. However, if ketone body production is unregulated and runs so fast it cannot be compensated for, there will be ketoacidosis.
This can happen in the case of diabetes mellitus type 1. When muscle and adipose cells cannot take in glucose, they have to break down fat into acetyl-CoA and then ketone bodies. The elevated glucose level in the blood will cause glucose to spill into the urine. This will increase diuresis by osmosis, which makes the acidosis even worse.
Alcohol causes dehydration, and alcohol dehydrogenase causes the NADH/NAD+ ratio to increase. This reduces the levels of pyruvate, which causes the pyruvate carboxylase reaction to slow down, which slows down gluconeogenesis. This causes the liver to be unable to produce enough glucose for the body, which will then start producing ketone bodies instead.
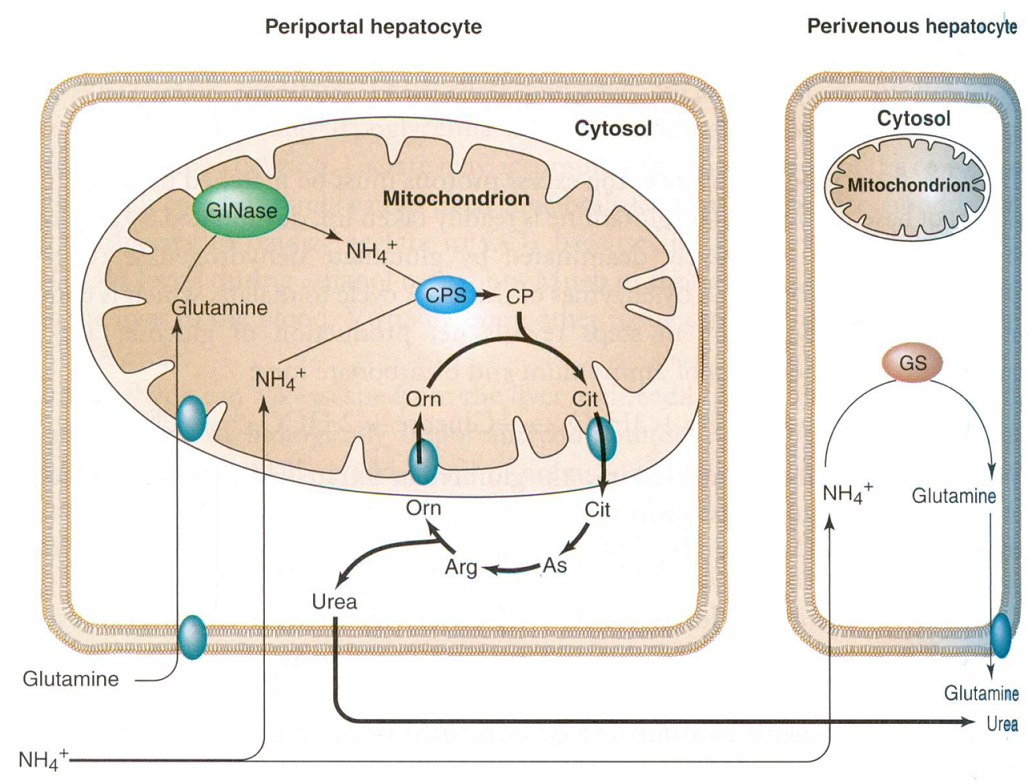
Ammonia
The hepatocytes in the liver uses two different enzymes to get rid of excess amonia, depending on where the hepatocytes are in the liver. Hepatocytes found around the central veins in the liver, perivenous hepatocytes, get rid of ammonia by incorporating it into glutamate using the glutamine synthetase enzyme. Hepatocytes found around the portal vein in the liver, the periportal hepatocytes, get rid of ammonia by incorporating it into carbamoyl phosphate, using the enzyme carbamoyl phosphate synthetase 1.
Kidney
The kidney can compensate for a mild acidosis with this reaction:
2Glutamine + 3O2 + 6H2O –> Glucose + 4HCO3– + 4NH4+