Table of Contents
Page created on January 8, 2022. Not updated since.
This and the next two topics are a mess. It’s difficult to understand which abnormalities go under which category (“abnormality of position/engagement/rotation”), as the lectures don’t talk much about them, they are inconsistent as to how they group the abnormalities and how they use the different terms, and other sources use the different terms to mean different things. I think I cracked the code (took days), but please leave a comment if you disagree or heard differently on the exam.
Abnormalities of foetal attitude
I’m not sure whether it should rather be included under any of the other topics or whether they expect us to talk about this at all. However, these abnormalities are explicitly mentioned in the corresponding topic for German programme, and they’re mentioned under “Tartási rendellenességek” in this presentation from Semmelweis. “Tartási rendellenességek” is the Hungarian name for this topic.
Introduction
In obstetrics, the foetal attitude refers to how flexed the foetal neck is. In normal cases, the neck is completely anteflexed so that the foetus’ chin is on its chest. This allows the smallest diameter of the foetal head to enter the pelvis, which gives the fewest mechanical problems with descent and delivery.
Abnormalities of foetal attitude refer to abnormalities of the degree of flexion of the foetal head. These include:
- Military presentation
- Brow presentation
- Face presentation
These may occur in case of preterm infants, if the umbilical cord is coiled around the neck, etc.
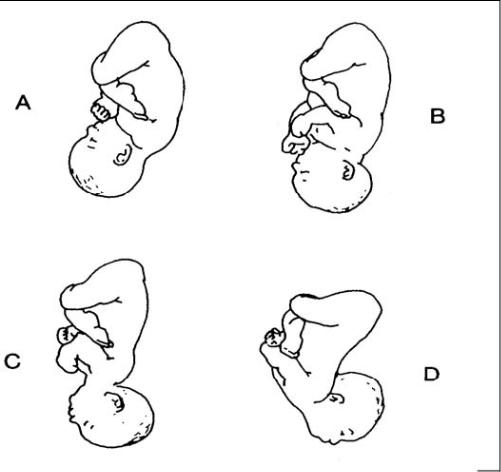
A – normal. B – military presentation. C – brow presentation. D – face presentation. From https://brooksidepress.org/ob_newborn_care_1/?page_id=475
Intrapartum, the foetal attitude can be determined by palpating the fontanelles, suture lines, and features of the foetal face.
Military presentation
In military presentation (also called sincipital presentation), the neck is lightly retroflexed. The diameter of the foetal head which must pass the pelvis inlet is no longer the smallest (but not the widest). The foetus may still be delivered vaginally. Vacuum extraction may be required, as well as early, large episiotomy.
Brow presentation
In brow presentation, the neck is moderately retroflexed. This causes the widest diameter of the head to enter the pelvic inlet first. This causes absolute mechanical obstruction, preventing vaginal birth and necessitating C-section.
Face presentation
In face presentation, the neck is completely retroflexed (hyperextended). The diameter of the foetal head which must pass the pelvis inlet is not the smallest (and is the second widest, between military and brow). The foetus may still be delivered vaginally, but only if there is adequate room in the pelvis. C-section may still be necessary.
Abnormalities of foetal position
This is what our English lecture calls “foetal position”. However, it does not include any abnormalities, it just explains what it means.
Introduction
In obstetrics, the foetal position means the relationship between a predetermined point of reference of the presenting part (occiput, mentum, sacrum, etc.) and the mother’s pelvis. In more simple terms, it reflects how the foetal head or buttocks is oriented within the birth canal. Knowing the foetal position is important before attempting operative delivery.
The position is described in relation to the mother’s left or right, and, optionally, in relation to the mother’s anterior or posterior. The position can be determined during labour by physical examination, feeling for landmarks such as the anterior fontanelle, posterior fontanelle, and ears. Each reference point has the possibility of four positions.
In occiput presentation (which uses the foetal occiput as the reference point):
- Left occiput anterior (LOA) – foetal occiput is directed towards mother’s left, anterior side
- Left occiput posterior (LOP) – foetal occiput is directed towards mother’s left, posterior side
- Right occiput anterior (ROA) – foetal occiput is directed towards mother’s right, anterior side
- Right occiput posterior (ROP) – foetal occiput is directed towards mother’s right, posterior side
In breech presentation (which uses the foetal sacrum as the reference point):
- Left sacrum anterior (LSA)
- Left sacrum posterior (LSP)
- Right sacrum anterior (RSA)
- Right sacrum posterior (RSP)
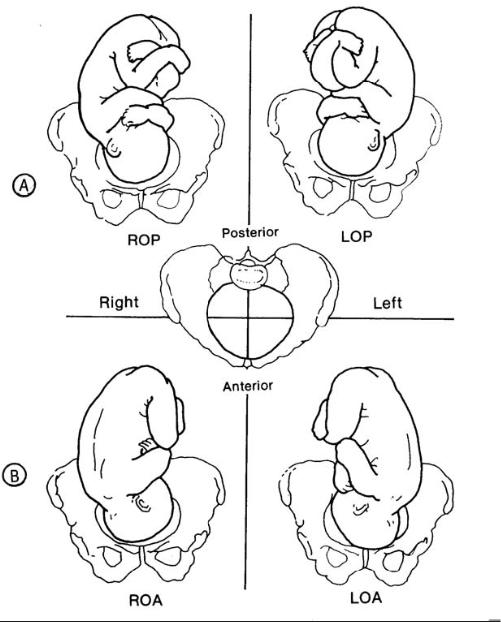
The four possible positions in occiput presentation. From https://brooksidepress.org/ob_newborn_care_1/?page_id=475
Occiput anterior
Occiput anterior, whether left or right (LOA or ROA), is the normal position and allows for the easiest delivery. LOA is more common than ROA.
Occiput posterior
Occiput posterior, whether left or right (LOP or ROP), makes labour more difficult and longer lasting. In many cases, it spontaneously rotates to occiput anterior during labour. If it does not, the condition is called persistent occiput posterior and is described in B27.
Thank you so much for the great clarification, been pulling my hair out for days too trying to know what belongs where <3
Glad it wasn’t just me! I hope I got it right in the end. It only took multiple days and searching the internet in three different languages. But that’s to be expected when studying for an exam, right? 🤷