Table of Contents
Page created on January 8, 2022. Last updated on December 18, 2024 at 16:57
Abnormalities of the foetal engagement
Introduction
In obstetrics, engagement refers to when the presenting part of the foetus passes the pelvic inlet. At this point, the foetus has reached the so-called 0 station. Once the foetus is engaged, it does not go back up. Abnormalities of foetal engagement include asynclitism and “high longitudinal position”.
Asynclitism
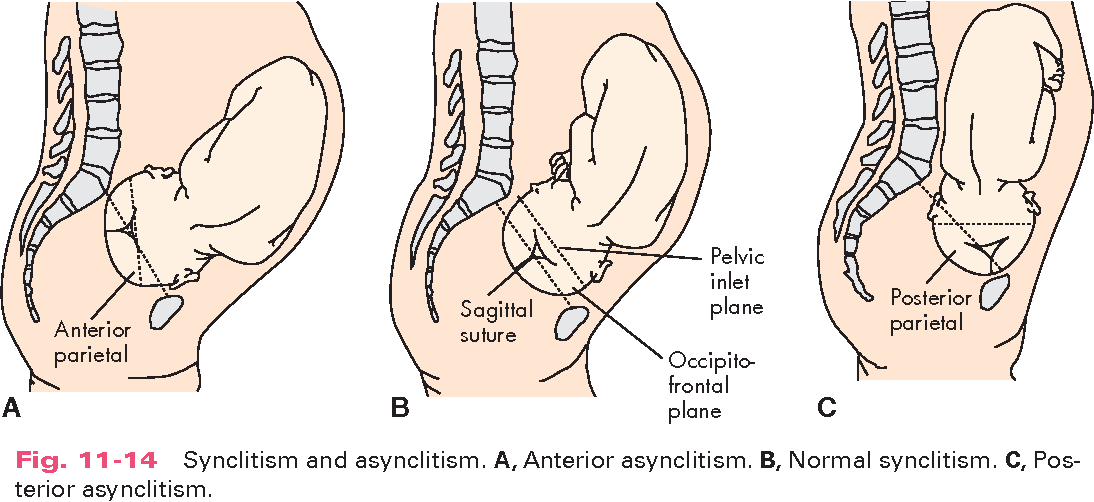
In synclitism, the plane of the biparietal diameter is parallel with the plane of the pelvic inlet, which makes the sagittal suture of the foetal head lie exactly midway between the pubic symphysis and the sacral promontory. This is the normal.
Asynclitism refers to when the head of the foetus is in an oblique position with the head tilted toward one shoulder. Asynclitism can be anterior or posterior. In anterior asynclitism, the head is tilted toward the sacrum, making the anterior parietal bone the presenting part. In posterior asynclitism the head is tilted toward the pubic symphysis, making the posterior parietal bone the presenting part.
Anterior asynclitism is also known as Naegele obliquity and posterior asynclitism is also known as Litzmann obliquity.
Asynclitism is associated with foetal malrotations, especially transverse and occipital posterior. It may be diagnosed based on vaginal examination and ultrasound.
From https://www.semanticscholar.org/paper/Labor-and-Birth-Processes-Learning-Objectives-Key-Lowdermilk/5ec0bc30878487ba055ef9a80c7ec7894a214757/figure/6
Anterior asynclitism is not a contraindication for vaginal delivery, but it will prolong the delivery.
Posterior asynclitism makes vaginal delivery impossible, as it causes absolute mechanical obstruction. C-section is required.
High longitudinal position
I’m not sure this is important, as it’s not mentioned in our lectures or found anywhere on the English internet really, but it’s explicitly mentioned in the corresponding topic for German programme, and it’s mentioned on Hungarian websites under “abnormalities of foetal engagement” (“Beilleszkedési rendellenességek”. It’s called “hoher Gegenstande” in German and “magas egyenes beilleszkedés” in Hungarian).
High longitudinal position or high sagittal position refers to when the sagittal suture of the foetal head is aligned along the antero-posterior diameter of the maternal pelvis. We distinguish two types, occipito-sacral high longitudinal position (foetal occiput facing the maternal sacrum) and occipito-pubical high longitudinal position. Occipito-pubical is more common.
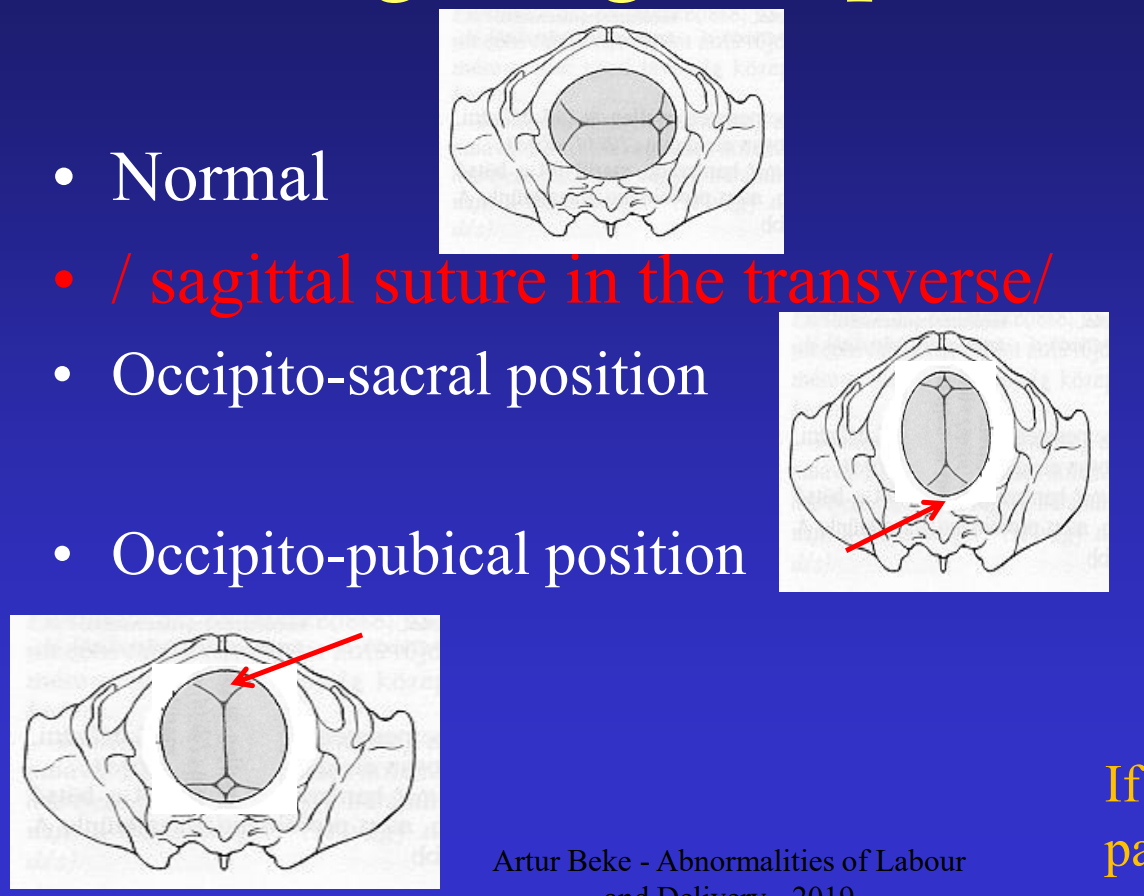
From top to bottom: Normal, occipito-sacral high longitudinal position, and occipito-pubical high longitudinal position. From https://semmelweis.hu/noi1/files/2019/10/abnormalities_of_labour_and_delivery.pdf
The head cannot pass the pelvis in this position, and so the position must be rotated. This can be attempted by telling the mother to change position, from left to right or vice versa, from lying to standing or standing on all fours, etc. If nothing helps, C-section is necessary.