Table of Contents
Page created on October 18, 2018. Last updated on December 18, 2024 at 16:57
Adrenergic receptors
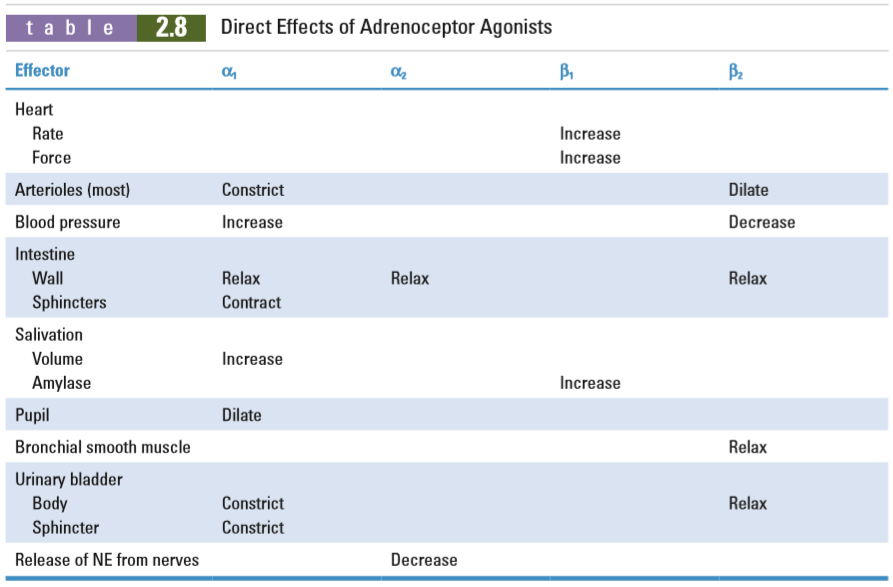
Three types of alpha adrenergic receptors exist, α1A, α1B and α1D (a C type was discovered but it turned out to be the same as the A type). Each of these subtypes are found in different tissues and have slightly different effects. However, the subtypes are highly homologous, so there is significant overlap.
α1A is mostly found in the bladder. α1B is mostly found in vasculature.
Phaeochromocytoma
Phaeochromocytoma is a cancer of the adrenal medulla which synthesizes large amounts of catecholamines. They bind to α1 receptors, causing vasoconstriction and severe hypertension.
It’s treated surgically but medical treatment is necessary to prevent catecholamine release during surgery. α1 receptor blockers and beta blockers are used.
Alpha blockers (α-receptor antagonists)
Compounds
- α1A receptor antagonists
- Tamsulosin
- Alfuzosin
- α1B receptor antagonists
- Doxazosin
- Terazosin
- (Prazosin)
- Non-subtype-selective α1-receptor antagonists
- Urapidil
- Non-selective α-receptor antagonists
- Phenoxybenzamine – (irreversible α-blocker)
- (Phentolamine)
- α2 receptor antagonists
- (Yohombine)
Phentolamine is rarely used. Doxazosin and terazosin have longer half-lives and are therefore now preferred instead of prazosin, which was the first drug in this class. Yohombine has no clinical use.
Indications
α1A receptor antagonists are preferred over other alpha blockers to relax the urethral sphincter in case of prostate hyperplasia, easing urination.
α1B-selective antagonists may also be used to ease urination in prostate hyperplasia. They can also be used to treat hypertension (but never as a first or even second-line option).
Urapidil may be used to treat hypertensive crisis.
Phenoxybenzamine (together with a beta blocker) is used to prevent catecholamine release from phaeochromocytomas before and during surgery.
Side effects
Side effects of all alpha blockers include postural hypotension, constipation, and possibly reflex tachycardia.
Phenoxybenzamine is a “dirty” drug, meaning that it blocks other receptors too, like histamine, acetylcholine and serotonine receptors. It also causes more reflex tachycardia than other types of alpha blockers.
Beta blockers (β-receptor antagonists)
Compounds
Beta blockers can, like alpha blockers, be classified according to their specificity:
- Non-selective beta blockers
- Propranolol
- Sotalol
- β1-selective beta blockers
- Atenolol
- Bisoprolol
- Esmolol
- Metoprolol
- Nebivolol
- Combined alpha- and beta blockers
- Carvedilol
- Labetalol
- Beta blockers only used topically (for the eye)
- Timolol
- Betaxolol
- Non-selective with intrinsic sympathomimetic activity (partial agonists)
- (Alprenolol)
- (Oxprenolol)
Beta blockers are very commonly used drugs and very worthwhile to learn well.
Because the β1 subtype is the one responsible for the cardiac effects, β1-selective beta blockers are often called “selective” or “cardioselective” beta blockers.
Alprenolol and oxprenolol are partial agonists and not pure antagonists. This gives them a milder beta-blocking effect than the pure antagonists. We used to think that this was beneficial in elderly but nowadays we know that that is not true, and so they have no use.
Indications
Beta blockers have many indications. Only the cardioselective beta blockers and the combined alpha and beta blockers are used for the following (cardiological) indications:
- Hypertension
- Angina pectoris
- After acute myocardial infarction (To prevent cardiac death after AMI)
- Chronic heart failure
- Arrhythmias
Propranolol has some specific indications:
- Tremors
- Migraine prophylaxis
- Portal hypertension
- Thyroid storm
- Prevention of oesophageal variceal bleeding
So does labetalol:
- Hypertensive emergencies
- Hypertension in pregnancy
Topical beta blockers like timolol and betaxolol are used to treat glaucoma.
Mechanism of action
Beta blockers treat hypertension not by causing vasodilation, but by blocking β1-receptors, causing decreased chronotropic and inotropic effects on the heart, reducing renin release and decreasing sympathetic activity centrally. All these effects indirectly decreases blood pressure.
This also decreases strain on the heart, which is why they’re used in heart failure. By decreasing the strain on the heart they also improve the symptoms in angina pectoris.
By blocking β2 adrenergic receptors β2-blockers decrease the production of aqueous humour, decreasing the intraocular pressure and relieving glaucoma.
Nebivolol is special because it induces NO release, causing vasodilation.
Combined alpha- and beta-blockers have additional vasodilating effects in addition to their beta-blocking effect and are therefore especially useful in hypertension.
Side effects
- Bronchoconstriction
- Is a contraindication for asthmatics, COPD patients
- Cardiac depression
- Can worsen acute heart failure (but helps chronic HF)
- Bradycardia
- Hypoglycaemia
- Because adrenaline releases blood glucose
- Especially in diabetics
- Cold extremities
- Due to loss of β-receptor mediated vasodilation in skin
- Nightmares
- Only for propranolol
The cardioselective beta blockers don’t cause vasoconstriction, bronchoconstriction or hypoglycaemia.
Pharmacokinetics
Metoprolol and propranolol are frequently used but have short half-life. Depot preparations exist for these drugs which circumvents the short half-life.
Most beta blockers are orally absorbed and undergo first-pass metabolism, and there is often significant interpersonal variance in the degree of first-pass metabolism. This makes the oral bioavailabilty highly variable.
Esmolol is special because it’s inactivated by enzymatic hydrolysis, giving it a very short half-life.
Contraindications
- Bradycardia
- AV block
- Cardiogenic shock and acute heart failure
- Hypotension
- Phaeochromocytoma (when given without alpha blockers)
- Giving beta-blockers alone to a person with phaeochromocytoma would block noradrenaline and adrenaline’s blood pressure-lowering effect on the beta-receptors, which would cause a net increase in blood pressure
- Asthma (not for cardioselective drugs)
- Pregnancy (except labetalol)
in the lecture, they have mentioned the complete opposite for urapidil and alfuzosin, they said that urapidil is basically alpha 1 A antagonist and alfuzosin is the non subtype selective antagonist, this is confusing
I just checked this year’s lecture on adrenergic antagonists, and I can not find what you’re saying on it. From what I can find, the lecture agrees with what I’ve written.
Hello greek.doctor.
Can you please expalin how A & NA lower BP when acting on beta receptors.
Thanks alot for your great website .
Adrenaline and noradrenaline increase BP when acting on beta receptors by stimulating the myocardial contraction and the heart rate, which increases the cardiac output.
thanks
Hey Nik ! Actually Yohimbin is used against erectile dysfunction 😉
From what I can find, it has very little medical use, although there is some evidence it could be slightly effective for erectile dysfunction. It’s more of an over-the-counter thing.
Hi!
Pheochromocytoma is a cancer of the adrenal medulla not the cortex 🙂
Yes
Hi! I was just wondering where you found the different contraindications for beta antagonists. Because when it comes to pheochromocytoma, the book it says that the best way to treat it is by giving both alpha and beta antagonists together. So how is it then contraindicated when giving beta antagonists?
It’s contraindicated to give them alone, because then you block the blood-pressure reducing effects of catecholamines (mediated by beta receptors), so that catecholamines only act on alpha receptors, which cause vasoconstriction and increase blood pressure. But you’re right, in combination they’re essential for the treatment of phaeochromocytoma.
hi nick ,
in topic 14 , you mentioned that drugs based on the their effect, may overlap . can you explain more about overlaping ?
for example , we can use phenoxybenzamin to ease urination , (but we dont since it,s not it,s primary function)
you mean this by overlapping ?
ps, thanks for the topics.
Hey!
Yes, that’s what I mean. Overlapping can occur in many drug classes but mostly those affecting the autonomic nervous system.
Timolol is a non-selective antagonist, not partial agonist 🙂
Fixed + more
Hey
How was microbio ? How did u prepare for it? Can u pls share some experience?
Thank you
I didn’t think people were interested in that, so I wasn’t going to write a post about it, but since you’re asking will I do it.
Hi
When will you take pharma ?
Are you gonna update more notes for it ?
Pleaseeee
Thank you ☺️
Hey!
I have pharma the 8th of January and micro the 2nd. As soon as I finish micro will I write more pharma notes.