Page created on November 28, 2018. Last updated on April 18, 2022 at 16:18
Grading and staging
It’s important for physicians to be able to communicate information about tumors in a standard, unambiguous way. By creating criteria, we can more easily determine the clinical behaviour of the tumor. To do this, we created two description protocols for cancers: grading and staging.
Grading of a cancer describes its degree of differentiation, i.e. how similar the cancer cells are to the corresponding healthy types of cell. A cancer is said to be well-differentiated if e.g.:
- It is epithelial in origin and produces keratin
- It is glandular in origin and produces gland-like structures
- Its cells show low degree of pleomorphism
- Not a high number of mitotic figures can be seen
Well-differentiated tumors are less aggressive generally, so the more well-differentiated a tumor is, the lower its “grade”. A low-grade tumor is well-differentiated, a high-grade tumor is poorly differentiated or even anaplastic. We can divide tumors into 2, 3 or 4 “grades”:
|
Four-tier grading |
Three-tier grading |
Two-tier grading |
||||||
| Grade 1 | Low grade | Well-differentiated | Grade 1 | Low grade | Well-differentiated | Grade 1 | Low grade | Well-differentiated |
| Grade 2 | Intermediate grade | Moderately differentiated | Grade 2 | Intermediate grade | Grade 2 | High grade | Poorly differentiated | |
| Grade 3 | High grade | Poorly differentiated | Grade 3 | High grade | Poorly differentiated | |||
| Grade 4 | Anaplastic | Anaplastic | ||||||
Which system we use depends on the type of tumor.
Staging is another system that is has more clinical value than grading. The most common system is the TNM system, which describes the size or extent of the tumor (T), the involvement of lymph nodes (N) and whether there’s metastasis or not (M). The system works like this:
| T | N | M | |||
| Tx | Tumor can’t be evaluated | Nx | Lymph nodes can’t be evaluated | M0 | No distant metastasis |
| T0 | No evidence of tumor | N0 | No tumor cells in sentinel lymph node | M1 | Metastasis to distant organs |
| Tis | Carcinoma in situ | N1 | Tumor cells present in sentinel lymph node | ||
| T1 | Size and extension of tumor on a scale from 1-4 | N2 | Between N1 and N3 | ||
| T2 | N3 | Tumor cells has spread to distant or numerous regional lymph nodes | |||
| T3 | |||||
| T4 | |||||
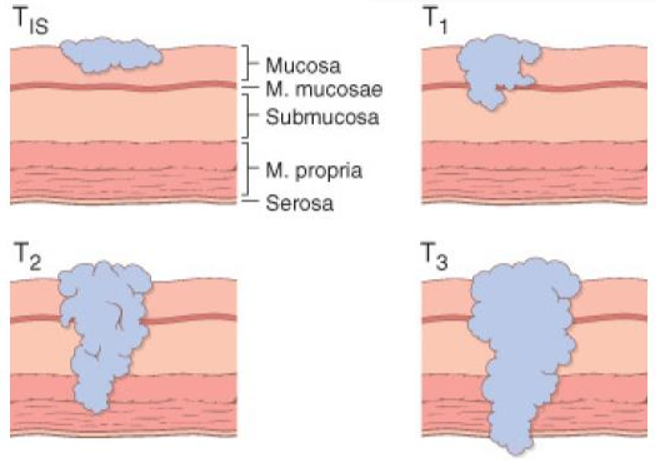
So a colorectal cancer which had spread to the submucosa, has spread to numerous lymph nodes and has no metastases would be T1 N3 M0.
Laboratory diagnosis of cancer
High-quality clinical information is very important in the diagnosis and treatment of cancer. Some non-cancerous conditions, like radiation damage of skin and mucosa, or the healing process of bone, can look like cancer under the microscope. An examination can only have as high quality as the specimen to be examined, so the specimens must be properly acquired and preserved.
Sampling is important. There are many sample techniques which we can use to get tissue samples, like:
- Excision biopsy is a type of biopsy done during open or laparoscopic surgeries.
- True-cut biopsy
- Fine-needle aspiration biopsy is less invasive than other biopsies, and is used in sampling palpable lesions of breast, lymph nodes, thyroid or salivary glands. If the structures are deep can the FNAB be guided by ultrasound or CT
- Exfoliative cytology, or cytological smears are used to collect cells shed from body surfaces, like the cervix (Pap smear), mouth or bladder.
Appropriate preservation of the specimen is important. Formalin is normally used, but glutaraldehyde and freezing may also be used. It’s important that fixation is done as soon as possible. Freezing the sample doesn’t perfectly conserve the tissue structure, but it’s quick and doesn’t require chemicals, which could interfere with some samples. Freezing is commonly used during surgery to make quick histological slides in order to find the border between tumors and healthy tissue.
Ancillary techniques are molecular techniques that can assist in diagnosing cancer. Important techniques are:
- Immunohistochemistry (IHC) uses antibodies conjugated with colourful substances to identify cell surface proteins, intermediate filaments and cell products.
- Intermediate filaments like cytokeratin, vimentin and desmin can be used to distinguish between epithelial and mesenchymal tumors in undifferentiated tumors.
- Tissue specific antigens like PSA and thyroglobulin can show the origin tissue in metastatic tumors
- Some molecules have prognostic and therapeutic significance, like HER2, c-kit, ER (oestrogen receptor) and PR (progesterone receptor)
- Flow cytometry can be used to measure cell characteristics, like
- DNA content
- Membrane proteins
- It’s also useful to identify T and B-cells
- Polymerase chain reaction (PCR) amplifies a given DNA sequence. It’s useful to identify gene translocations, mutations and deletions
- (Fluorescent) in situ hybridization, (F)ISH is used to study gene and chromosome alterations, like gene translocations and amplifications
- Comparative genomic hybridization (CGH) is used to compare two genome samples to identify gains or losses of chromosomal regions
- Karyotyping is the basic method of studying chromosomes. Spectral karyotyping is used to detect chromosomal changes