Table of Contents
Page created on February 17, 2019. Last updated on December 18, 2024 at 16:57
Written by ms. worldwide, edited by Nikolas.
Benign lesions
Polyps can also occur in the stomach. There are many types of polyps, and some of them are not neoplastic, and is typically seen in some diseases.
Non-neoplastic polyps
- Hyperplastic polyps
Almost all polyps in the stomach tend to be hyperplastic polyps, and its associated to chronic gastritis, both with or without H. pylori.
The polyps are usually 1-2 cm big and located in the antrum as multiple polyps. The risk of developing into malignancy is low, but it increases if the polyps are bigger than 2 cm.
- Fundic gland polyps
Fundic gland polyps can occur sporadically or in persons with familiar adenomatous polyposis (FAP) and are usually located in the fundus and the corpus of the stomach. These polyps are well circumscribed and are composed of dilated irregular glands which are lined by parietal and chief cells. The interesting part is that their occurrence has increased due to increased use of proton-pump inhibitor therapy, which will result in the increase of gastrin release and glandular hyperplasia by gastrin.
These polyps usually don’t develop into something malignant, except if the patient has FAP since the polyps appear in a younger age and more numerous, with some dysplasia.
- Hamartomatous polyps
These kinds of polyps consist of disorganized cells and tissue which are usually found at the site of where the polyps lie. They are mostly part of polyposis syndromes, like Peutz-Jeghers syndrom.
- Inflammatory fibroid polyp
These polyps are basically submucous granulomas with infiltration of eosinophils, and they have a round whitish appearance with a gum-like consistency.
- Xanthoma of the stomach
Recall that a xanthoma is a “lipid island”, which can also be found on the eyelids and around the eyes. Having them in the stomach is most common in Japan and can be due to bile reflux. They have no significance clinically.
Adenomas in the stomach
The adenomas are considered rare, and the chances of getting them increase with age and with the different populations. Men have also 3 times higher risk of getting them. Adenomas mostly occur in patients with a history of chronic gastritis with atrophy and intestinal metaplasia and are usually located in the antrum. Since they show a morphology similar to intestinal columnar epithelium, we say that they show an epithelial dysplasia, and they can be graded by the Vienna classification (not included here).
The risk of it turning into adenocarcinoma increases when the lesions are bigger than 2 cm.
Gastric adenocarcinoma
Introduction and epidemiology
Gastric cancer is a cancer of elderly, mostly men, and it’s the fifth most common cancer worldwide. It is more common in Asian countries like Japan and Korea, as well as certain regions in Africa and South America.
It causes no or only nonspecific symptoms in the early stages. If diagnosed early, the prognosis is excellent, but at the time of diagnosis, 50% of cancers have already spread and are incurable, which leads to a poor prognosis overall.
The mortality of this cancer is higher in the countries with low prevalence because screening is not performed as often as in high-prevalence countries. Therefore, the cancer is often discovered too late.
Etiology
- H. pylori gastritis or other atrophic gastritis
- Diet rich in nitrates or salts
- Alcohol
- Nicotine use
- Epstein-Barr virus
- Gastric adenomas
- Previous partial gastric resection
Plant-based diet is protective against gastric cancer.
Clinical features
The early symptoms are absent or non-specific like dyspepsia (indigestion), abdominal pain, and nausea, until the patient reaches the later stages with weight loss, different bowel habits, anaemia and haemorrhage.
Pathology and classifications
95% of cases of gastric cancer are adenocarcinomas. The carcinoma is usually located in the antrum, followed by corpus and fundus.
We distinguish “early” and “advanced” gastric cancer. Per definition, “early” gastric cancer infiltrates no deeper than the submucosa but even early cancer can give metastasis to the lymph nodes, while “advanced” cancers infiltrate the muscularis propria and deeper.
Lauren classification
We can use the Lauren classification which separates the gastric cancers into intestinal and diffuse types according to their location in the stomach and their gross and histological morphology.
The intestinal type has glandular structures. It has a better prognosis than the diffuse type. This type can be classified as high grade or low grade depending on whether the glandular structures show poor differentiation or well differentiation, respectively.
The diffuse type has a special cell type called signet ring cells spread diffusely across the mucosa. These cells have their nuclei compressed on the periphery of the cell, and they have large mucin-containing vacuoles in the cytoplasm. They can be hard to find on biopsy because they’re so diffusely spread. This type is more aggressive and has a worse prognosis than the intestinal type.
Borrmann classification
Macroscopically, we can see 4 different types of gastric cancer according to the Borrmann classification:
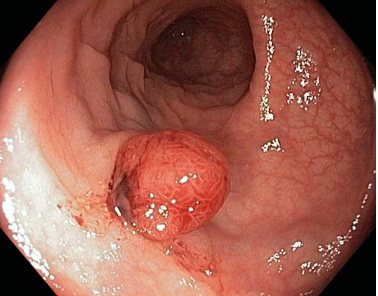
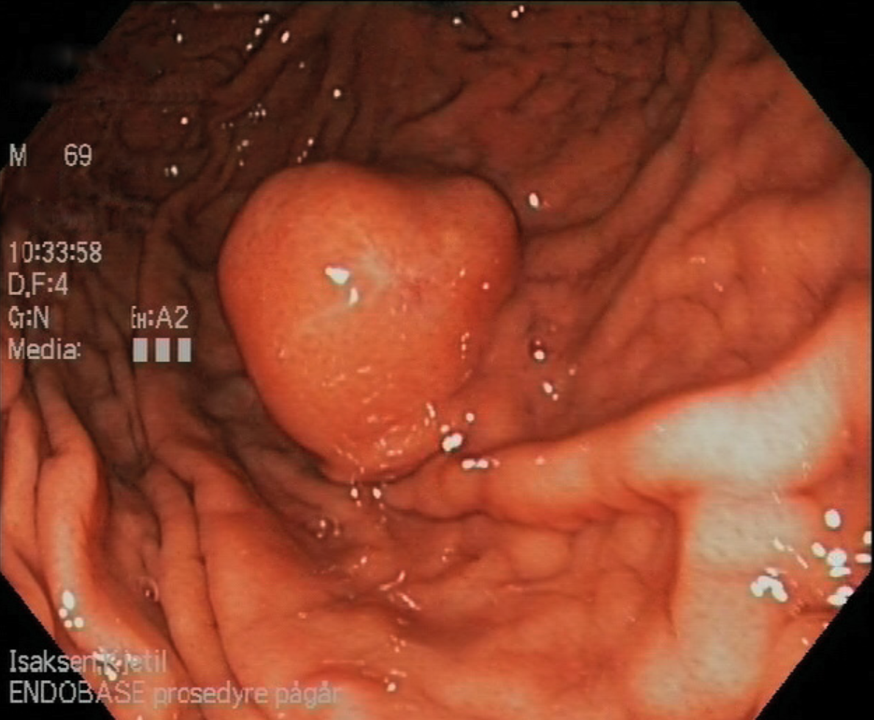
- Polypoid type – Protrudes into the lumen like a polyp
- Fungative type – Protrudes and has ulcerative surface
- Ulcerative type – Non-protruding with ulcerative surface
- Diffuse growth type – Diffusely thickened gastric wall (linitis plastica)
Linitis plastica is the end-stage of diffuse type gastric cancer, where the entire stomach is affected by the cancer. This leads to a rigid, non-distensible, “leather bottle-like” stomach.
Metastatic spread
Gastric adenocarcinoma often spreads to skeleton, liver, lung, brain, and the peritoneum. The Virchow lymph node, the left supraclavicular lymph node, is the most common site of gastric cancer metastasis.
Diffuse type of gastric adenocarcinoma may metastasise to both ovaries (bilateral), forming a so-called Krukenberg tumour.
Other gastric cancers
Gastrointestinal stroma tumor (GIST)
This type of tumor is the most common mesenchymal tumor from the interstitial Cajal-cells. It can occur anywhere in the GI-tract, but is most commonly found in the stomach, followed by the duodenum.
The C-kit gene, which encodes for a tyrosine kinase, is often mutated in the patients with GIST. The mutated tyrosine kinase becomes constitutively activated, causing nonstop activation of the downstream effects and progression to cancer.
Morphologically, the tumor can either be submucous, subserous or intramural. The submucous one is often ulcerated and polypus.
Treatment is by surgery with or without the addition of tyrosine kinase inhibitor (imatinib), a drug which blocks the mutated tyrosine kinase.
Gastric lymphomas
Lymphomas can arise in every tissue, but the stomach is the most common site of extranodal lymphoma. However, it’s still one of the rarest malignancies that you can have there. The lymphomas include:
- MALT lymphoma
- DLBCL – diffuse large B-cell lymphoma
We will discuss these briefly.
MALT lymphoma of the stomach
MALT lymphoma is a cancer originating from B-cells in the MALT. The risk factor is H. pylori, which secrete the endotoxin CagA that leads to B-cells proliferation and autoreactive B-cells. These events eventually lead to a lymphoma. Treatment is by treating the H. pylori infection, which causes the lymphoma to regress.
DLBCL – diffuse large B-cell lymphoma
DLBCL is more aggressive than MALT lymphoma, and can either be primary (de novo), or secondary following the transformation of a MALT-lymphoma.
With m. muscularis, do you mean tunica muscularis or muscularis mucosae? love u <3
Corrected.
Love you too <3
“What are the differences between an early and an advanced gastric cancer? The earlier cancers infiltrate only the *submucosa* but can also give metastasis to the lymph nodes.”
Did you mean to write “The earlier cancers infiltrate only the *mucosa*”?
Nope, check the lectures. UpToDate also defines early gastric cancer as “invasive gastric cancer that invades no more deeply than the submucosa, irrespective of lymph node metastasis (T1, any N).” I changed the paragraph to be more accurate, though.