Table of Contents
Page created on May 23, 2019. Last updated on September 22, 2021 at 17:28
General
On the ECG repolarization is characterised by the ST segment and T-wave. Any abnormality of cardiac repolarization will be seen on the ECG as abnormal ST segments or T-waves.
Repolarization abnormalities can be primary or secondary in etiology. A repolarization abnormality is primary if the preceding depolarization (QRS complex) is normal and secondary if the QRS complex is abnormal.
Primary ST segment abnormalities
The J point is the point where the QRS complex transitions into the ST-segment, the exact point where the QRS complex ends. This point is important for evaluating the ST segment.
ST elevation:
The ST segment is usually isoelectric, meaning that it lies at level with the PQ-interval. We consider the ST segment to be elevated if the ST-segment is more than 0.1 mV (one small square) above the level of the PQ-interval 80 ms after the J-point. If there is tachycardia, the value 60 ms should be used instead of 80.
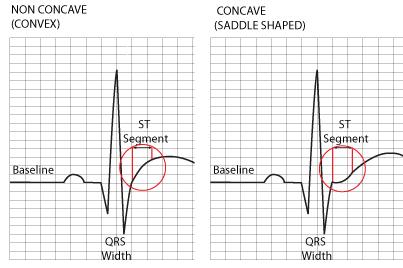
We distinguish two types of ST elevation:
- Convex or dome-shaped ST elevation
- Concave or ascending ST elevation
From https://www.rcemlearning.co.uk/references/st-elevation-without-infarction/
The different types of ST elevations are present in:
- Convex ST elevation
- Acute myocardial infarct – in the leads representing the region of the infarct
- Prinzmetal angina
- Ventricular aneurysm
- Concave ST elevation
- Normal physiological variant
- Pericarditis – in most leads simultaneously
Mild concave ST elevation is usually nonpathologic.
ST depression:
Likewise, we consider the ST segment to be depressed if the ST-segment is more than 0.1 mV (one small square) below the level of the PQ-interval 80 ms after the J-point.
We distinguish four types of ST depression:
- Ascending ST depression
- Horizontal ST depression
- Descending ST depression
- Scooped ST depression

The different types of ST depressions are present in:
- Ascending ST depression
- Normal – during physical activity
- Horizontal ST depression
- Myocardial ischaemia
- Angina pectoris
- Descending ST depression
- Severe myocardial ischaemia
- Left ventricular strain
- Coved ST depression
- Digitalis effect (not digitalis toxicity)
Primary T-wave abnormalities
The normal T-wave is:
- Concordant in extremity leads
- Positive in chest leads
The main abnormality of the T-wave is that it is inverted, i.e. it’s discordant in extremity leads or negative in chest leads. T-wave inversion very unspecific, meaning that it occurs in very many conditions and therefore isn’t really diagnostic for any one condition. Here are some conditions that can cause primary T-wave inversion:
- Ischemia
- Infarct (coronary T)
- Pericarditis
- Myocarditis
- Fever
- Infection
The most important primary T-wave abnormality is the coronary T. The coronary T is a tall, pointed negative T-wave that occurs in the acute phase of acute myocardial infarct.
Secondary repolarization abnormalities
In secondary repolarization abnormalities the depolarization of the ventricles is abnormal in some way, which causes the ventricular repolarization to be abnormal as well as a result.
Conditions with secondary repolarization abnormalities:
- Bundle branch blocks
- Hemiblocks
- WPW syndrome
- Ventricular hypertrophy
- Beats of ventricular origin
The clinical importance of secondary repolarization abnormalities is that they cannot be evaluated, or, in other words, they cannot be taken as a sign of something. Here are some examples:
- ST-elevations in bundle branch blocks
- ST-depressions in WPW
- Inverted T-wave in ventricular extrasystoles
In bundle branch blocks, WPW and ventricular extrasystoles the depolarization of the ventricles doesn’t occur normally, so the repolarization will be abnormal as well. In our example we can’t interpret the ST-elevation in a bundle branch block or the ST-depressions in WPW as signs of ischaemia; they’re simply the consequence of abnormal depolarization.
Ventricular hypertrophy causes secondary repolarization abnormalities. Furthermore, ventricular hypertrophy also causes secondary repolarization abnormalities.
It’s so important it should be mentioned twice!
Or not
Smart a$$es are annoying. It’s so important for Nikolas to know that I’ll mention it twice, smart a$$es are annoying!
(:
(: