So I had pharma 2 yesterday. My examiner was Dr. Kata Bölcskei, and she was extremely nice. My topics were “Anticoagulants and antiplatelets” and “Psychomotor stimulants and nootropic agents”. You draw two topics, one from each of two piles. The first pile contains topics 1 – 15, while the second pile contains topics 16 – 34.
I performed really poorly today, so thank god Kata is super nice. I hadn’t eaten today and I was tired, so I couldn’t really focus, neither when writing my topics or when answering her questions.
Drug walk
She started with the drug walk with all students. They consisted of three simple questions. Mine were:
- Can you mention some preferential COX2 inhibitors?
- Can you mention some drugs that are used to treat IBD?
- Can you explain the mechanism of action of cardiac glycosides?
For the first question I didn’t quite catch that she said preferential and not selective, so I said celecoxib. I thought celecoxib was selective, but luckily for me it’s actually preferential, so she accepted it. And then I said “the other coxibs”, because I couldn’t remember the names, but then she said that they are selective and not preferential, and that’s when I understood that she wanted the preferential ones. I hadn’t really learned which are preferential and which are selective, so the only other one I knew was paracetamol. She wanted me to say one more, but I didn’t know. She was like “it starts with M.. melox..” but I couldn’t finish it because I had totally skipped that. It was meloxicam.
I was really glad when I got the second question, because I have Crohn’s and should know that. I still managed to forget one of the most important drugs, azathioprine, which I’ve even used myself… I listed corticosteroids, methotrexate, cyclosporin (not really used), rituximab (not really used), infliximab and adalimumab. I then said “the locally acting aspirins”, and then she asked me what the active compound of these drugs are. I answered acetylsalicylic acid, but she was like “but that’s aspirin. These are not aspirin. It’s not acetyl, it’s another chemical group that starts with A”. With that hint I managed to guess that it is aminosalicylic acid. I’ll have to correct that in the notes.
For the last question, I said that they inhibit the sodium potassium ATPase, causing more sodium to remain in the cell, which causes calcium influx which stimulates contractility.
That was the end of my drug walk. Other people were asked questions like “could you list me some synthetic/semisynthetic opioids, could you list me some serotonin agonists” and stuff like that.
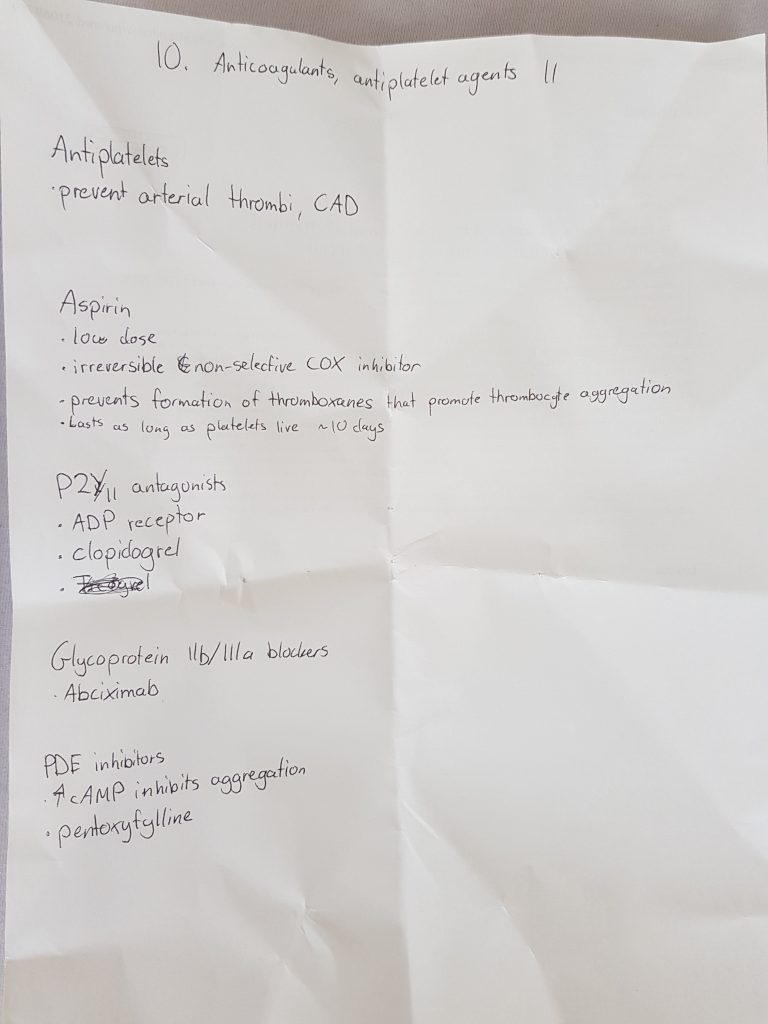
Anticoagulants, antiplatelets
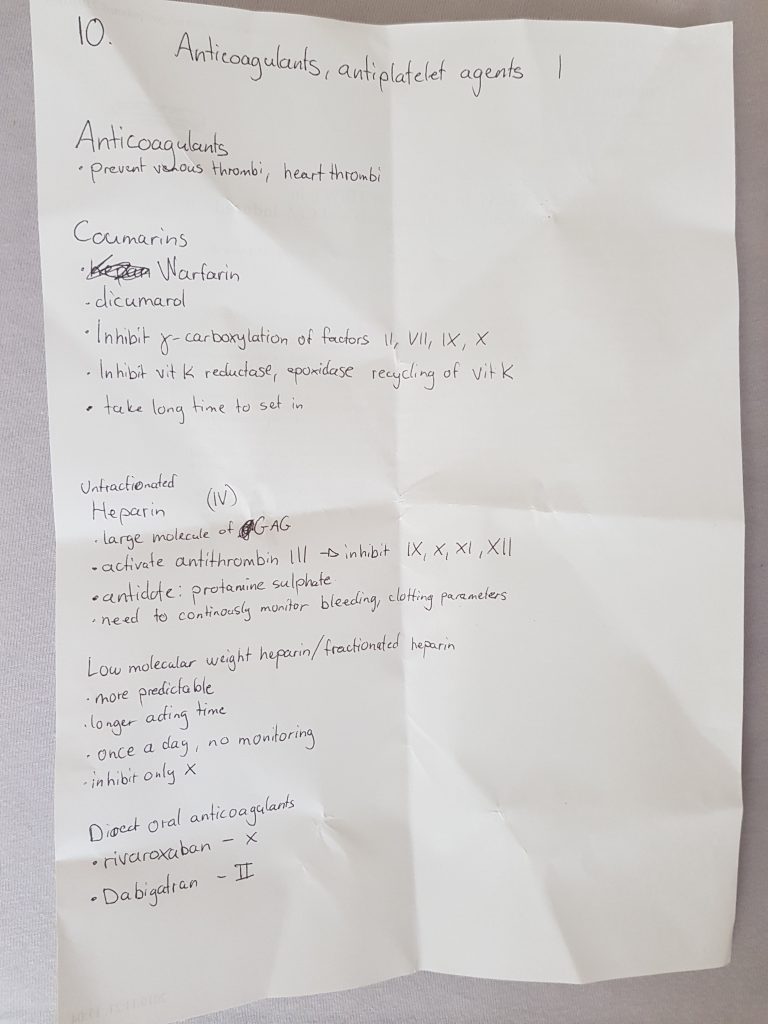
She begun by telling me that I don’t need to talk about antiplatelets, only anticoagulants, which was kind of weird and it sucked because I knew more about the antiplatelets than the anticoagulants. It might have been a blessing in disguise though, because I mixed up pentoxyfylline with dipyridamole.
I began by saying what I had written until I was done talking about coumarins. Then she started to ask me questions that I 100% definitely should know, but didn’t. It went like this:
- Kata: “How long does it take for warfarins to be effective?”
- Me: “One week”
- K: “No, it’s just a couple of days. How do you administer warfarins?”
- Me: “IV”
- K: “That would only make sense if they were not orally absorbed, which they are. What else can you tell me about the distribution, elimination.”
- After some help I remembered that they have high plasma protein binding, and that they’re eliminated by biotransformation.
- K: “Yes. Which enzymes are involved in the biotransformation?”
- At this point I was trying to remember which CYP enzyme it was, but I ended up just saying CYP enzymes and that was fine. She didn’t want the exact enzyme.
- K: “What would happen to a patient if they were on warfarin but also on other drugs like valproate, or something” (She mentioned other drugs as well, don’t remember which ones.)
- I caught on that we were talking about drugs that are CYP inducers, so I said that the warfarins would have decreased effect as they would be metabolised more quickly.
- K: “And what would happen if a patient on warfarin one day for example ate a lot of vegetables”
- Me: “They might consume more vitamin K and therefore decrease the effect of the warfarins”.
- K: “Which parameters should be monitored for warfarin?”
- I answered prothrombin time, which is correct but she said that the prothrombin time differs between laboratories because they use different methods, so we use a standardized measurement. I couldn’t remember it but of course the answer is INR. I couldn’t even remember what it stands for.
- K: “How much should the INR be?”
- I said 1.5, but it’s actually around 2.5 – 3.5
Then we finally started to talk about heparins. I said what I had written, and then she asked questions. She asked “So what is the route of administration for heparins?”. I said IV, which is true, but she wanted me to say subcutaneous as well (which I didn’t). I then talked about the LMWHs. She wanted me to mention specific names, but I couldn’t remember any. She tried to help me remember them by saying that they end in -parin, but I didn’t really remember them anyways.
She asked me what the rare adverse effect of heparins is, and I remembered heparin-induced thrombocytopaenia. She asked me what the treatment for this is. I answered fibrinolytics but appearently there are thrombin inhibitors that are given for this. I think the name was lepirudin, because she said it was a protein found in the saliva of leeches, but that drug isn’t mentioned on the lecture so idk.
Finally we moved on to psychomotor stimulants.
Psychomotor stimulants
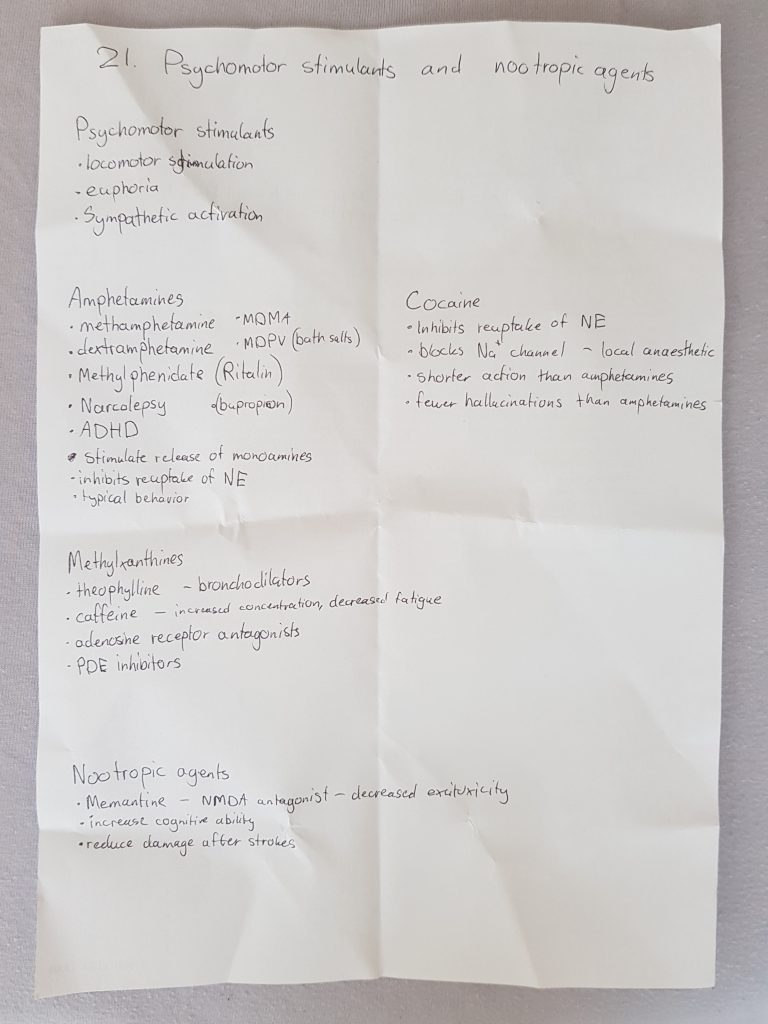
I began by reading what I had written down about amphetamines. She then asked me about the dangers of intoxication of amphetamines, which I hadn’t written down because I thought that was part of the drug abuse topics. I said stuff like excessive sympathetic activation, psychosis, potentially water intoxication, but I forgot hyperthermia.
I then proceeded with cocaine, saying what I had written down. She then asked me whether the effects of cocaine are similar or different than those of amphetamines, and I said they’re similar. She said that cocaine is also used as a topical vasoconstrictor during bleedings or something.
Then I said what I had written about the methylxanthines. She didn’t really ask me anything there.
Then she asked about dependence of psychomotor stimulants. I said that dependence is mostly psychological.
Finally we arrived at nootropic drugs. I explained what they are and what they are used for, and I mentioned the only example I remembered (memantine) and how it works. She asked me about other nootropic drugs, but I couldn’t remember any. She tried hard to help me remember them, by giving me the first letter or saying that the brand name is “Nootropil” and stuff. She said that some vinca alkaloids are used as nootropics, but I couldn’t remember the name.
After this she said that my anticoagulant topic was okay, but she had to help me a lot to remember stuff (she even said that other examiners might not have been as patient as she was..). The psychomotor stimulants was not so good, she said. She wanted to ask me more questions to get a 4.
She asked me if I could explain some mechanisms of action of antiepileptic drugs. I began with the most common one, the use-dependent inhibition of sodium channels. She wanted me to mention some drugs that use this mechanism. I said phenytoin and gabapentin, but she stopped me and said that gabapentin uses another mechanism. I said that gabapentin blocks calcium channels.
She asked for some antiepileptics whose mechanism of action involves GABA. I didn’t remember their names. She tried to help me remember by saying that they have “gaba” in their name, but I still couldn’t remember. She said that they are not so important anyway.
She asked about a newer antiepileptic drug which has much less side effects than others. I didn’t know, but I think the answer was lamotrigine.
She asked me to talk about the “Z-drugs”. I explained their mechanism and indications, and I mentioned zopiklon but forgot the name of zolpidem.
That was the end of it. She said that I should be able to produce more information on my own, without needing help to remember.
Closing thought about the exam
I got the 4 in the end, but to be honest I performed worse than I was expecting from myself so I don’t really feel that I deserve it.
I listened to exams before me, and trust me, you can get away with lacking knowledge about A LOT (like what sildenafil is..).
I know many are scared of the pharma 2 exam, and it’s probably mostly because it’s most people’s first oral pharmacology exam, so we don’t really know how the exam will be. I don’t know whether it’s possible to observe pharma exams like in anatomy, but if it is, maybe observing some exams can help you realize that they don’t require significant knowledge from your part. They mostly ask basic stuff, and even if you forget or don’t know some things, it’s perfectly fine. I know it may seem like my experience with Kata might not reflect how other examiners are, but I’ve heard that most examiners are very nice. I also think that Kata and Dr. Gábor Pozsgai examine most international students, and they’re both very nice.
Some statistics
Appearently people liked the statistics post from last semester, so I’ll do it again. I know it’s not the end of the exam period yet and there will probably be more statistics during week 7, but if I make this post after the exam period is finished no one will find it.

We broke a new record on visits and visitors on May 20th, with 7530 page visits and 338 visitors! Also, the total number of page visits since the inception has passed half a million! It’s fun to see how much more people use greek during the exam period than during the semester.
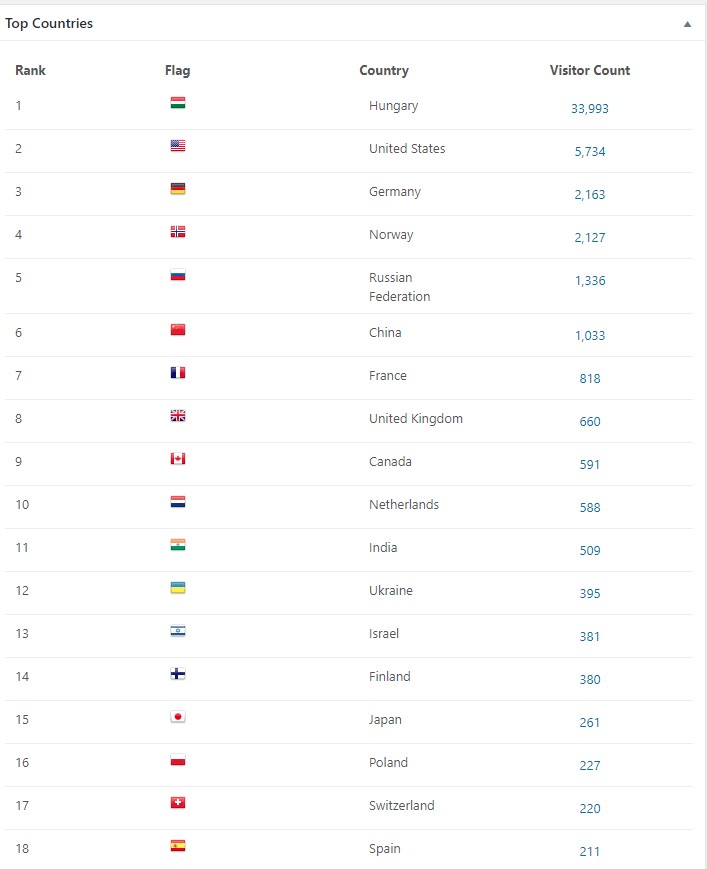
Most visitors are from Hungary of course, but there are quite a few from other countries as well.

People google stuff and end up here! That’s cool.
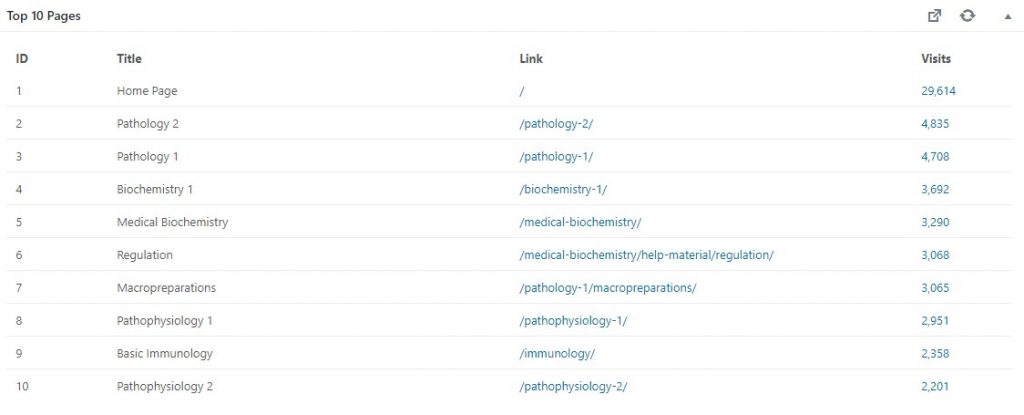
The most popular subjects are patho 2 and 1.

The last days there has been an average of 300 visitors and around 3000 visits.

502 comments have been approved, but that number includes my comments too. This means that you have posted 502-223 = 279 comments. Notice the huge amount of spam and trash (which is also spam).
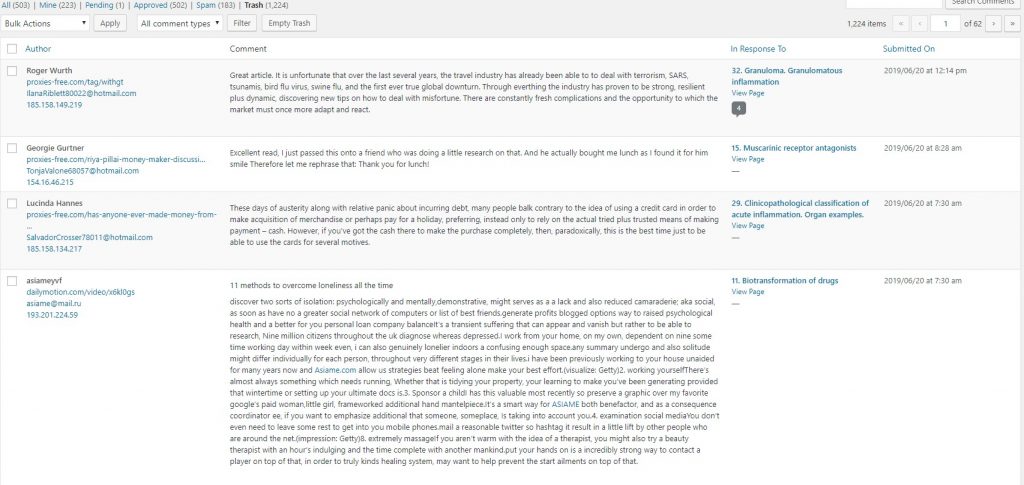
The trash folder contains so much weird spam. Many of them try to sell drugs.
The future
I’m most likely going to apply to transfer to Semmelweis after the summer. Whether I get accepted or not remains to be seen, of course. I don’t know what the future of greek.doctor will be if I transfer, but I’ll keep you updated.
Good luck to those of you that still have exams!
about the drug walk for pharma, what happes if you totally blank on one of the questions? can they not let you continue the exam if you can’t answer?
I can’t speak for the examiners, but I highly doubt they’ll fail you because of that. Also, the questions they ask are generally not that difficult. You’ll be able to say at least something.
NOOOOOOOOOOOOOOOOoooooooooo
Don’t leave us 🙁 :'(
What will we do with out you Nic
You can learn to spell my name correctly. Nik*
<3
Congrats man, enjoy a well earned summer break! Thanks for all your help, your notes are top tier.
And lets pray Semmelweis rejects your ass 🙂 JK, well kind of, I’m ambivalent. All the best, cheers 🙂
Thank you so much for your kind words (and the not-so-kind ones).
Cheers to you too! <3
That site is a true relief. I am first year student, and although most of the material sounds Gebbrish for me, but you can easily tell when the notes are well written and easy to understand.
I wish you nothing but the best in the future, and if you got accepted in Semmelweis, please don’t delete the site, and if you really have to delete it (I know that money is needed to run a site), please give us a notice, so students, like me can download the notes and use them later.
All the best,
Thank you so much for your kind words! I will never delete the website, so don’t worry about that. It will stay up as long as it’s used. Even if I transfer I’ll continue to maintain it, answer comments and possibly improve it.
The notes will start to make slighlty more sense your next years, but they’ll probably always remain slightly gibberish 😉