Page created on November 22, 2018. Last updated on December 18, 2024 at 16:56
Systemic lupus erythematosus is an autoimmune disease where virtually any organ in the body can be affected. It’s very clinically unpredictable, is relapsing and can have an acute onset or it can start slowly. It most commonly affects the skin, kidneys, serous membranes, joints and the heart.
The incidence of SLE varies considerably between groups. The most frequently affected group are black female Americans, where 1 in every 250 is affected. Females are 9 times more frequently affected than men. It mainly arises in the 20-30s, but it can start at any time of life.
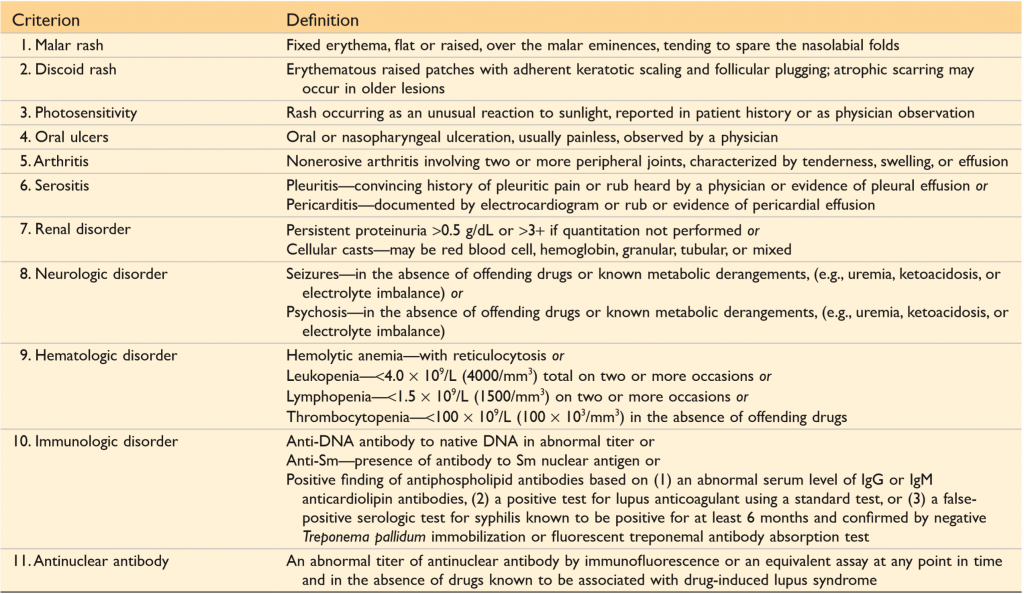
Because SLE can have such a vast variety of symptoms has the American College of Rheumatology developed a system of diagnostic criteria for SLE. 11 criteria exist, and if 4 or more of these are present can SLE be confirmed. The criteria are (not important to know but still):
Pathogenesis of SLE
SLE is a complex disease, meaning that many factors are involved in its development. They all include some loss of immunological tolerance. Here are some of the involved factors:
- Genes like HLA-DR2 or HLA-DR3 have an odds ratio of 2 to 3 for developing SLE. The presence of both alleles gives an odds ratio of 5. Genetic defects in genes for classical pathway complement proteins are also seen in some patients with SLE.
- Environmental factors like UV radiation, cigarette smoking and certain drugs increase the risk for SLE.
- Immunologic abnormalities exist in patients with SLE. Patients with SLE produce abnormally large amounts of an interferon called IFN-α. Toll-like receptor 7 and 9, which recognize RNA and DNA respectively, may be important to recognise nuclear antigens. Studies on B cells from patients with SLE show that these patients have defects in both central and peripheral tolerance
A model has been proposed to explain the pathogenesis of SLE. Environmental factors like UV radiation cause increased apoptosis of cells. The body fails to clear the nuclei of these cells, partly because of defects in the complement system, which assists in clearing. This means that there is an increased amount of nuclear antigens present. Several genetic defects lead to loss of immunological tolerance, causing self-reacting lymphocytes to be present in the body. B-cells recognize (with the B-cell receptor) and produce antibodies against nuclear antigens. B cells internalize the antibody-antigen complexes and use TLR7 and TLR9 to recognize the nuclear antigens. This causes them to produce more antibodies and to stimulate dendritic cells, which produce IFN-α which induces more apoptosis, causing a self-fuelling cycle.
Indeed, many anti-nuclear antibodies (ANAs) are found in the sera of patients with SLE. These antibodies target many different proteins inside the nuclei of cells, like double stranded DNA (dsDNA), a protein called Sm and histone proteins. However, anti-nuclear antibodies can be found in 5 to 15% of healthy people even, so these antibodies are not alone in causing SLE. ANAs can’t penetrate cells, meaning that they can only bind to nuclear structures that have been released from cells after the cell has died. When ANAs bind to nuclei of dead cells do they form histological LE bodies or haematoxylin bodies.
Certain antibodies against structures other than nuclear structures can be found as well. Antiphospholipid antibodies are present in approx. 50% of patients with SLE. These antibodies contribute to coagulation abnormalities. Antibodies against red and white blood cells and platelets are also usually present.
Most organ damage in SLE is due to immune complex deposition, meaning that SLE is partly a type III hypersensitivity. Recall that immune complex deposition usually occurs in the kidneys and in small blood vessels like in the skin. Skin and kidney biopsies in patients with SLE usually show heavy granular deposits of complement and immunoglobin. Immune complex deposition causes tissue damage by activating complement, the mechanism of which is explained here.
The antibodies against RBCs, WBCs and platelets cause type II hypersensitivity, where the antibodies opsonize the cells and platelets. Opsonized cells and platelets activate inflammation by the function of complement, and the cells are phagocytosed by phagocytes, leading to cytopaenias.
The antibodies against phospholipids lead to increased thrombosis, causing thrombotic episodes and possible spontaneous abortion. This is a manifestation of secondary antiphospholipid syndrome, the condition where antiphospholipid antibodies cause a hypercoagulable state.
Clinical manifestations
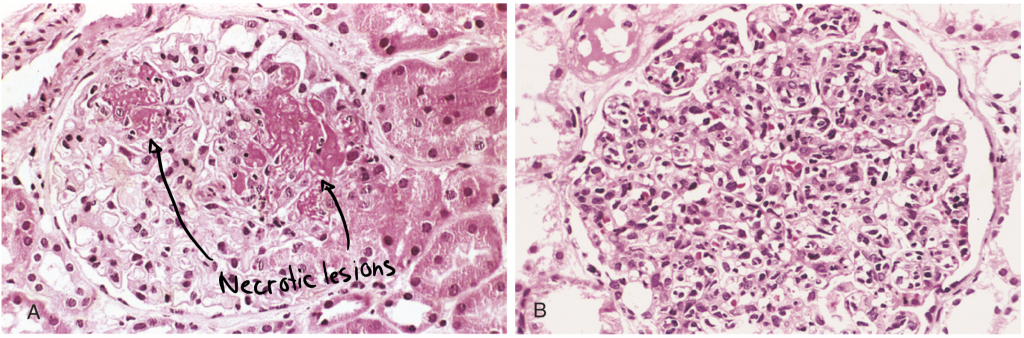
Recall from the topic about type III hypersensitivity that acute necrotizing vasculitis is a common symptom. It’s characterized by necrosis and fibrinoid deposits in vessel walls.
Kidney involvement is one of the most important clinical features of SLE. Renal failure is a common cause of death in these patients. Deposition of DNA-anti-DNA immune complexes in the glomeruli causes glomerulonephritis. The inflammation in the glomeruli may cause proliferation of endothelial, mesangial or epithelial cells, and possibly necrosis of the whole glomerulus.
The skin is commonly involved. A butterfly-shaped erythematous eruption on the face is characteristic for SLE. Similar rashes may be present on the extremities and on the trunk, and the rashes are worsened by UV light. Histological examination of the rash shows hydropic or vacuolar degeneration of the basal layer of the epidermis.

Joints are also sometimes affected, although the changes in the joint don’t usually cause visible change. Synovitis is common.
CNS abnormalities are common, often manifesting as cerebral microinfarcts and cerebral ischaemia. Symptoms include headaches, confusion, depression, seizures, vision problems and others. Pathogenesis could be proliferation of the tunica intima due to antiphospholipid syndrome, which occludes the arteries.
Heart involvement is normal. Both pericarditis, myocarditis and endocarditis can occur. The type of endocarditis is a special one called Libman-Sacks endocarditis, which is one of the major causes for non-infective endocarditis. It involves vegetation on the valves, most commonly the mitral valve. Nowadays will the treatment of SLE prevent the formation of Libman-Sacks endocarditis.
Atherosclerosis is increased in patients with SLE, which can cause coronary artery disease.
Splenomegaly is common. Perivascular fibrosis produces lesion with a special morphology, called onion-skin lesions.
Serous membranes like pericardium and pleura undergo fibrinous inflammation. Organization of the fibrinous exudate may cause hardening and opacification of the membranes.
according to Dr.House, it,s never lupus 😂
ps. thanks for your great website
Except when it is.
Thank you <3
Hey
I think under the clinical consequences of SLE “heart” it should be Lidman sacks and not Libman sacks
Hey!
Libman is correct.
https://en.wikipedia.org/wiki/Libman–Sacks_endocarditis