Here is the previous post. Unfortunately, I have bad news regarding the biyearly statistics. Sometime in March this year, the website started getting spammed, and it still is, every day. I don’t know why or how, but it happened. This luckily doesn’t cause any problems for the website, but it does skew the statistics because these spam visits are indistinguishable from visits from actual people. I’ve tried to implement measures to decrease spam visits, but they haven’t helped.
Because of these spamming bots, the visit count has increased drastically this semester, with the majority of visits now being from bots rather than actual humans. This makes it impossible to compare to previous semesters and to know the actual interest in the website. I’ll show you.
Statistics
As usual, a page “visit” refers to opening a single page on greek.doctor. A “visitor” is a unique person within that day. This graph includes the page visits from the week before the beginning of the semester until the last day of the exam period.
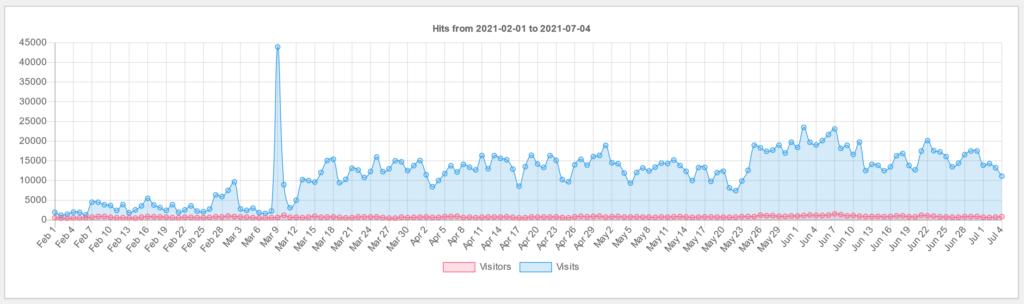
I’d say the numbers are valid and realistic up until the middle of March. Before the semester began there were approximately 400 daily visitors and 1300 visits. In the beginning of March, the number was approximately 500 and 1600, respectively. However, after the beginning of the spamming there are approximately 700 visitors and 16 000 visits every day. Note also the spam peak on March 9th, with 43 900 visits.
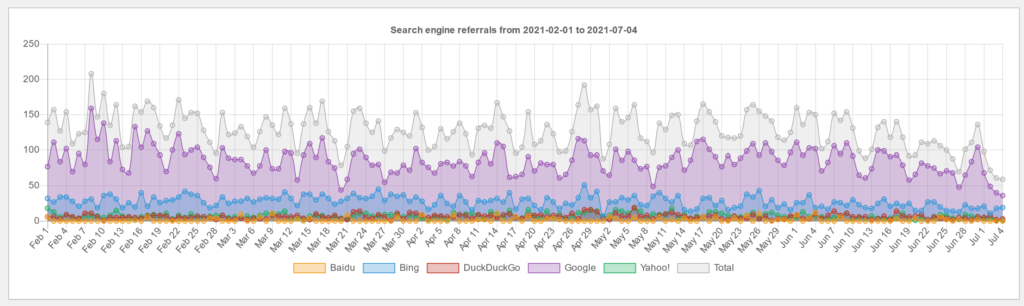
Search engine referrals are probably unaffected by the spamming. The numbers are pretty similar to last year.
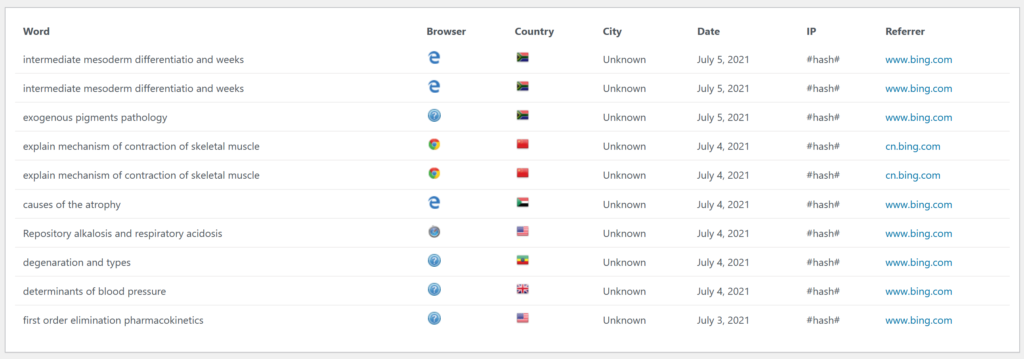
These are the last 20 search words people used before ending up at greek.doctor.
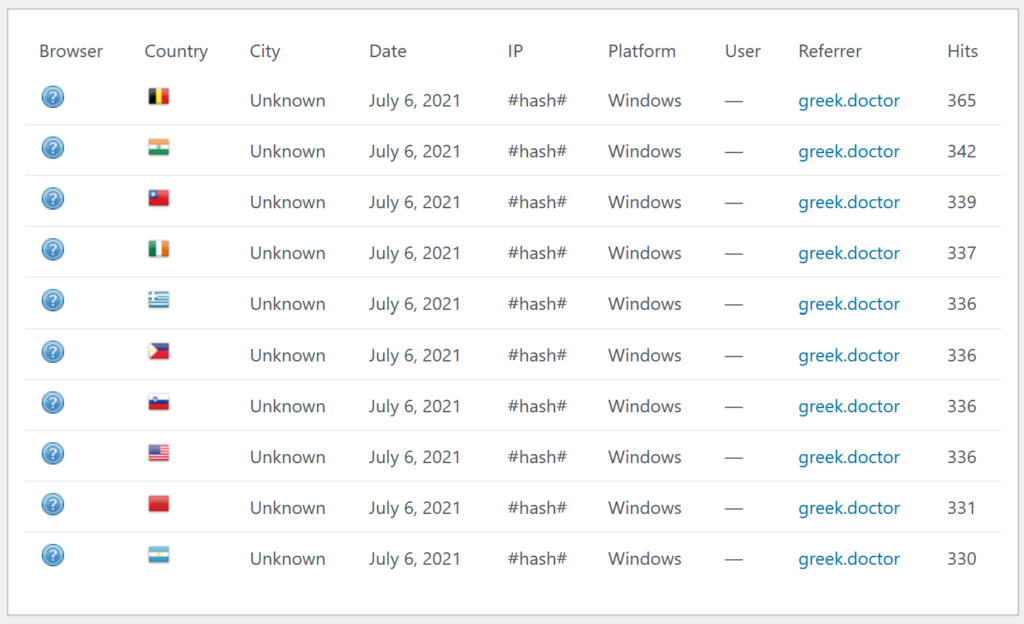
This statistic is one of the stronger proofs that the website is being spammed. It is the top 10 visitors of the website today. Compare it to the top 10 visitors from before the spam.
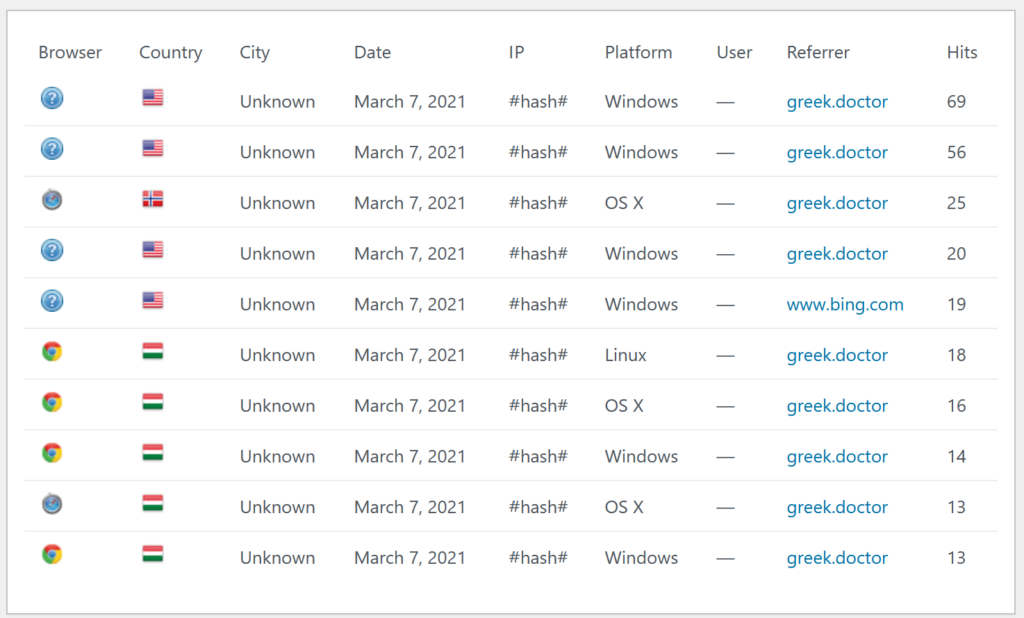
The top 10 visitors used to mostly be from Hungary, use modern browsers, and have sensible visits (hits) per visitor.
Comments
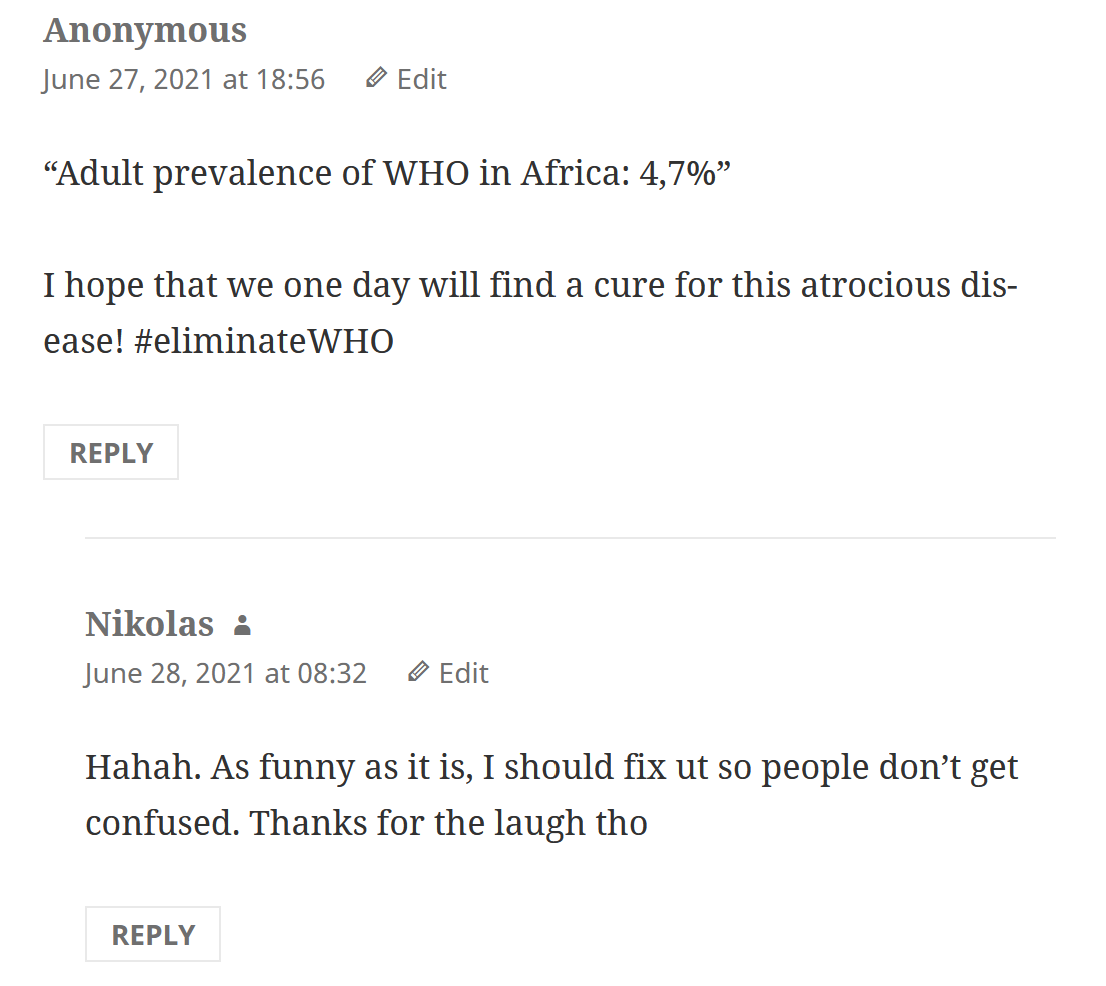
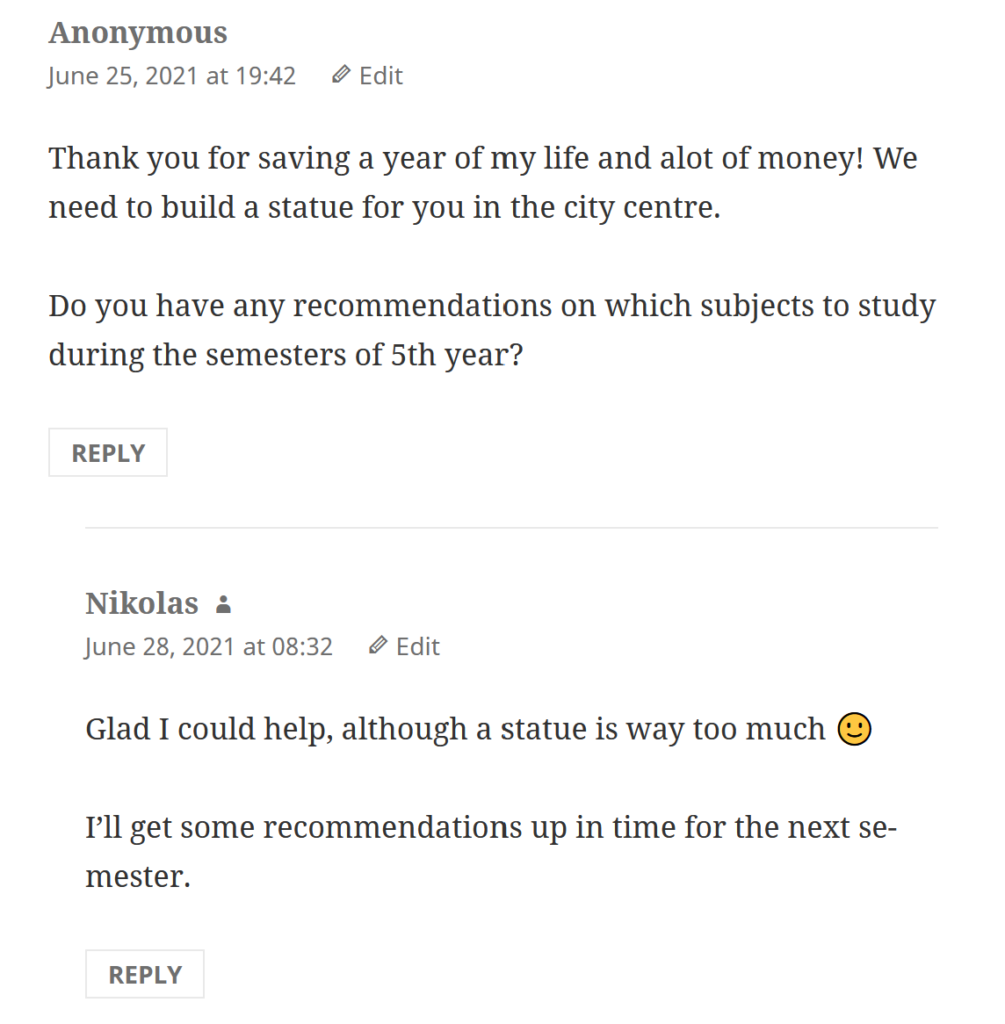
Time for a few fun comments!
Next semester
I plan to write notes for some of the subjects in 6th year. I’ll write a new post soon with which subjects I’m going to write for and when.
Until then, enjoy your summer!
My summer
In Norway, 6th year medical students can be hired to do doctor work, mostly in wards. There are very few positions available, much fewer than the number of students who are interested, so getting hired for a position is more of an exception rather than a rule.
I was extremely lucky this year and actually got a position! My position is at one of the bigger hospitals in Norway, Akershus University Hospital, which you might recognise from a certain tiktok. I’m going to be working 7 weeks in the cardiology ward, doing rounds on patients, discharging patients, doing paperwork, etc. I had my first day yesterday, but today was the first day where I was responsible for my own patients. I’ve gotten this period accepted as my 6th year internal med practice.
On this day I:
- Wrote my first ever prescription
- Did my first ever rounds
- Wrote my first ever application to the state for sick leave for a patient (who had an AMI)
However, I also managed to:
- Introduce myself as “Nikko” to one of the chief doctors
- Say “sorry for crushing your dreams” to a nurse who asked me if she could measure NEWS less frequently, making my collegues laugh at my choice of phrasing
- Misunderstand the computer system, making me think that blood culture on a septic patients had not taken for no good reason (while in reality they were taken)
- Need to work 1 hour overtime to get done with all my tasks
… but it’s all good, because a nurse told me that she thinks I’m doing a good job.