Rheuma MRTs are up. If you don’t know what the MRTs are, I’ve explained that in the beginning of the page.
Fun fact – rheuma means “stream”, “current” or “flow” in Greek.
I have both rheuma and cardio on Wednesday.
Rheuma MRTs are up. If you don’t know what the MRTs are, I’ve explained that in the beginning of the page.
Fun fact – rheuma means “stream”, “current” or “flow” in Greek.
I have both rheuma and cardio on Wednesday.
Here. Only 10 557 words this time. Not all topics are finished, as only the lectures will be asked in the test on Monday, not the seminars (I had already written some seminar topics before they told us that). The unfinished topics will probably remain unfinished.
Now what?
So at least 2 people were interested in a team for studying, so I made one. You can join it by entering the code 8eth6rg at the top of the teams window or by clicking the link here.
18696 words later, cardiology notes are done. Onco next! Hope to be done some time before the test.
Also, greek.doctor has a new member on the team, G cobra (real name Jørgen)! He has been part of it for some weeks now, and I’ve told him to write a post introducing himself, but he never did, so I’m doing it for him.
G has patho 2 now and contributes to the patho 2 notes while he is studying. He also responded to his first comment yesterday! Welcome <3
Another thing; would people be interested in having study sessions with me on Teams?
So I made a small recording of myself writing cardio notes. I’ve thought about doing it for a while, so people could get an impression of what I do when I write.
The video is quite long (40 min), but it spans almost three hours of writing. You can find the video here.
Surgery 1 notes are done, mostly, and are uploaded. Some topics, especially among the cardiac surgery ones, are short because the lectures don’t contain much information about it.
Surgery 1 is the only subject we must pass in fourth year to continue, so I figured it was a good place to start. Cardio is next.
I’ll continue to update the notes if necessary, during the semester.
The COVID-19 crisis needs no introduction. I’m sure you all know the economical situation the crisis has brought with it. We are looking at a second economic depression, equal to or worse than the one in the 30s. This crisis affects all levels of the education, and now also greek.doctor.
Because of this, I’ll now have to start taking payment for the use of greek.doctor. The price of running the website has increased with the crisis, and I also need to afford rent, food, heat and masks for my whole family for the foreseeable future.
Like all hospital and health institutions, greek.doctor will also change to code red, by changing the colour of the website from the familiar golden orange to firetruck red. This will remain until the COVID-19 crisis is over. I apologize for the inconvenience. I know it is quite the eyesore, but it’s important to signal the severity of the situation.
My intention with greek.doctor was never to make money, and my philosophy has always been to keep knowledge free and available. However, desperate times require changes. I cannot afford to continue to pay for the website in addition to my expenses, and it’s time I get something in return for spending all this time helping people.
Because the payment has to be delivered in person, from now on the website can only be used by residents in Pécs. I apologize for this, but I will have to be strict to uphold this rule. I have systems in place ready for this change. If you are a student at POTE but not currently in Pécs, you have to contact someone here who can deliver payment for you.
Payment has to be made up front on a per-day or per-week basis. I will not issue monthly access tickets, for safety concerns. Unfortunately, this is non-negotiable. I can give close friends a discount, but only up to 15%. Less close friends can get a discount of 5%.
Greek.doctor aims to be a legal business, so I have to write receipts. Receipts will be written in person and on paper. I have a pen but you have to bring the paper, as I can’t carry that much around (I suspect that a lot of receipts will be written). For the receipt to be official and follow regulations the paper has to be of high quality. Please refer to the copyshops and ask them for high quality, receipt-approved paper. I’ve already talked to the officials in the government to get a license to sell this product.
Due to virus transmission fears, and in accordance with the curfew, a minimum distance of 1,5 m must be kept when standing in line for a receipt. Please uphold this rule so we can avoid problems with the police. We don’t want that, and after all, it’s not really allowed to meet anyone during the curfew, so all of this is kind of shady. Please avoid taking space in the road while standing in line.
If you have questions regarding this, please send a letter adressed to me to Student Parcel Point, Szigeti ut 12, 7621 Pécs. I know this is a huge hassle but unfortunately I cannot afford to pay for my hotmail so I won’t be able to respond to emails. I have gotten special permission from POTE to collect any letters sent to the university adressed to me.
Domain names (like greek.doctor) cost money, and some are more expensive than others. The .doctor suffix is especially expensive, considering it’s meant for doctors. If the economical situation doesn’t change I might have to change the domain name to something cheaper. I have some ideas, but I won’t share them now. I will say that the cheaper domains are those that end in .xxx and .gay, so I might be forced to choose something like that. If you have good suggestions, share them in the comments.
Anyway, the price will be as follows:
– for one day of use: one kiss to my forehead
– for one week of use: two kisses to my forehead
These changes will take place from today (April 1st) and indefinitely.
I apologize for the inconvenience and I beg of your understanding.
Love
greek.doctor
I made a small page called “other useful sites” where I share some of my most used resources when studying.
Another exam period has ended. Hope it all went well for you. People like statistics, so I’m bringing ’em.
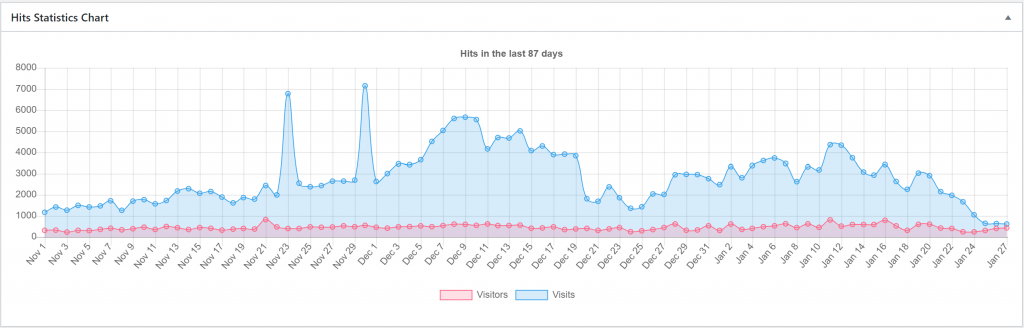
On the graph you can see how the daily visitor and visit count has been from November 1st until today. It’s fun to see the graph gradually increase during the semester as the exam period closes in. It peaks in the days before week 1 and during it, as people are frantically studying pharma, patho and biochem 1. Good to see that many people took the christmas time off. You can also see that there are still some visits when POTE has vacation, which is probably mostly students from other places in the world.
As most of the subjects I’ve written for are subjects people usually take in the first weeks, I think it’s natural that we see the highest numbers of visitors in the first weeks.
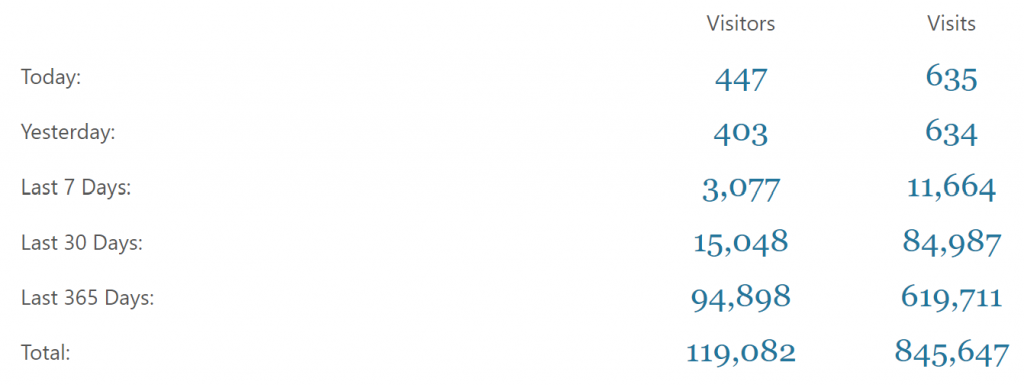
The peak number of daily visits was 5659 the 9th of December. The peak number of daily visitors was 809 the 11th of January, which I can’t really understand. It was a Saturday. During the exam period there were a total of 153 002 page visits. During the semester there were 153 806 page visits, but that’s including those robot peaks, so in reality the number should be around 144 000.
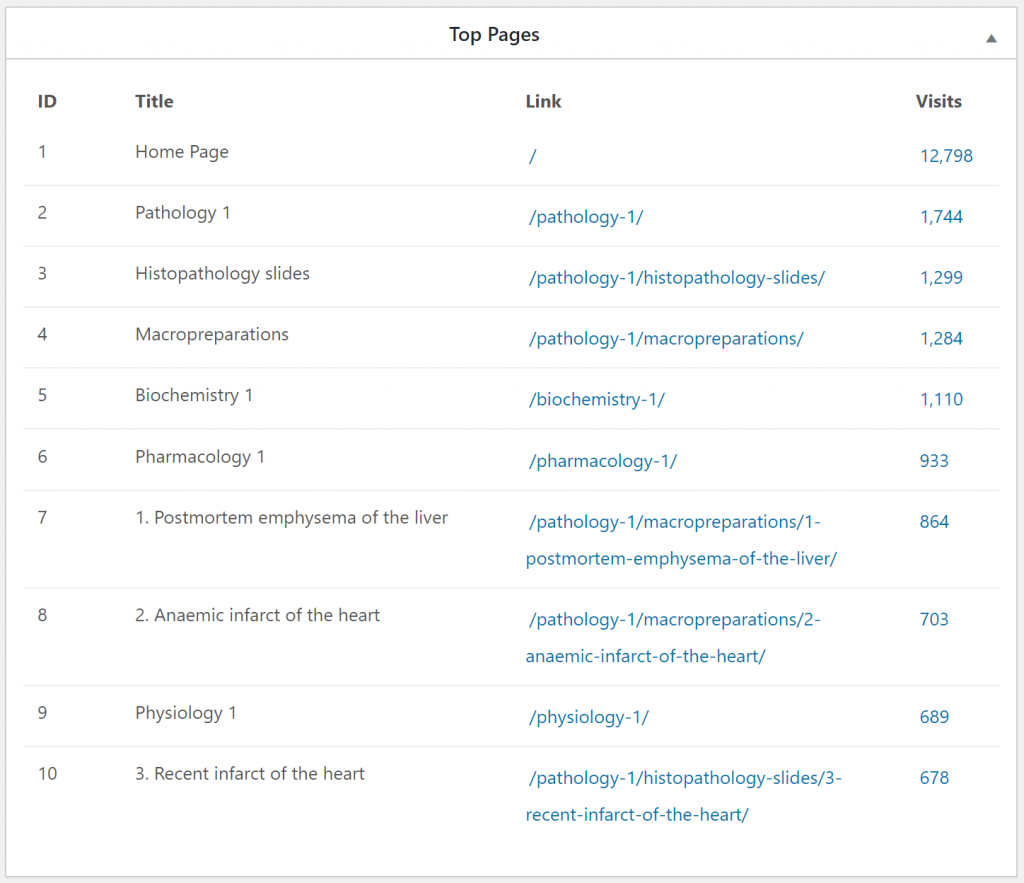
During the exam period these were the top visited pages. The visit numbers are for this exam period. Scrolling further down the list shows that the most popular pages are the histo slides and macropreps for patho 1.
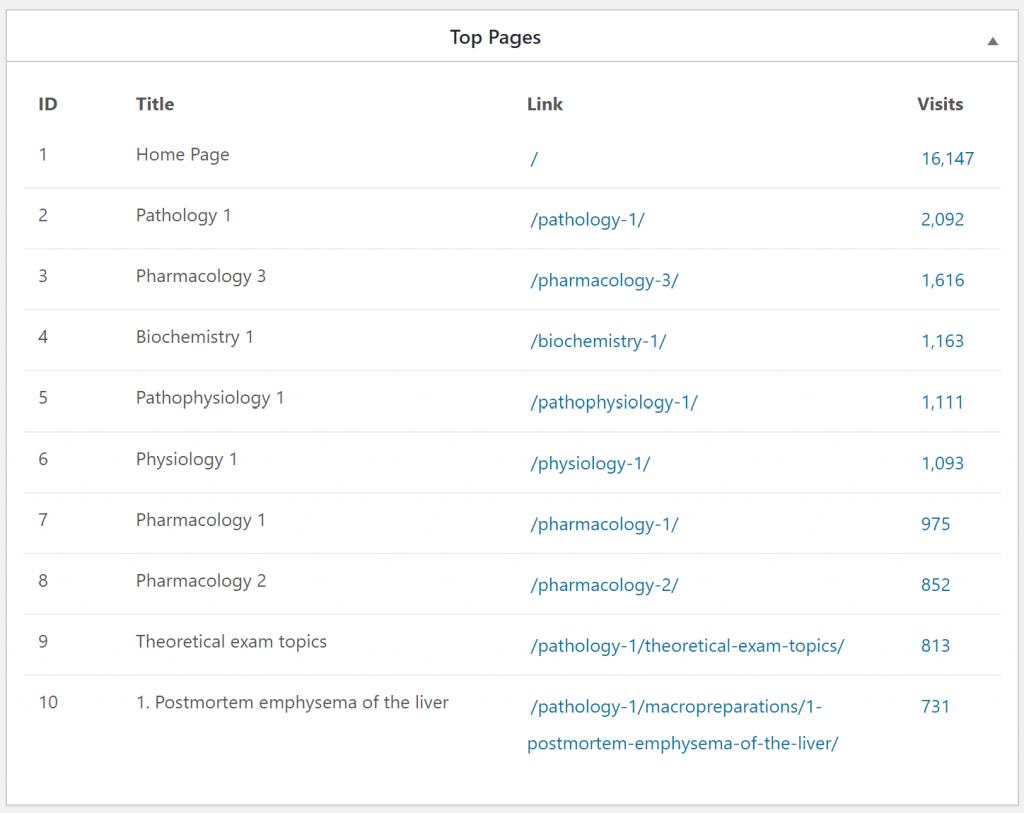
These were the top visited pages during the semester. I think this shows that people tend to study more generally across subjects during the semester, but during the exam period they study topics more specifically. Also that nobody studies macropreps and slides during the semester.

There are now a total of 788 comments on the website, 353 of which are mine. 788-353 = 435 comments are made by readers. I don’t have exact numbers, but the vast majority of comments arise during the exam period. I think I got 2 – 3 comments daily on average during this exam period.
Most comments point out mistakes in the notes, some ask for clarification, some ask for advice, but a few commenters are just here to flex. Here are some interesting comments.
I’ve run out of statistics, and if I were to share every interesting comment this post would go on forever.
See you next semester/exam period!
So I had derma yesterday. It’s been one week since radio, but I didn’t start studying before tuesday, so I really only studied three days. This is gonna be a long post.
I usually go through the topics orally with my girlfriend the day before the exam, and I did the same this time. However, I quickly noticed that I didn’t actually remember shit from any of the topics, not even the easy ones. It was thursday at like 22:00, so I didn’t have much time. I suddenly realized how fucked I was, which was a feeling I don’t usually feel before exams. The only thing I could do was to sit down and go through the whole curriculum again, which took me 3 hours. In other words, I didn’t get much sleep that night (only 4 hours).
At the day of the exam, we wait outside the library in derma department. I’m super tired from lack of sleep. A teacher comes and collects those who had to do the practical, while the rest of us waited. A secretary comes and tells us that the examiners today are Dr. Ágnes Kinyó and Prof. Rolland Gyulai. Ágnes comes a few minutes later and takes a few students in to the library to do the exam. I was still very stressed and I still wanted to go through my notes a few more times, so I didn’t go in as one of the first students.
The first student comes out not very long after, and says that she’s super nice. Great, I think, then I’ll probably pass at least. The next students say the same. Eventually, I go in and pick topics.
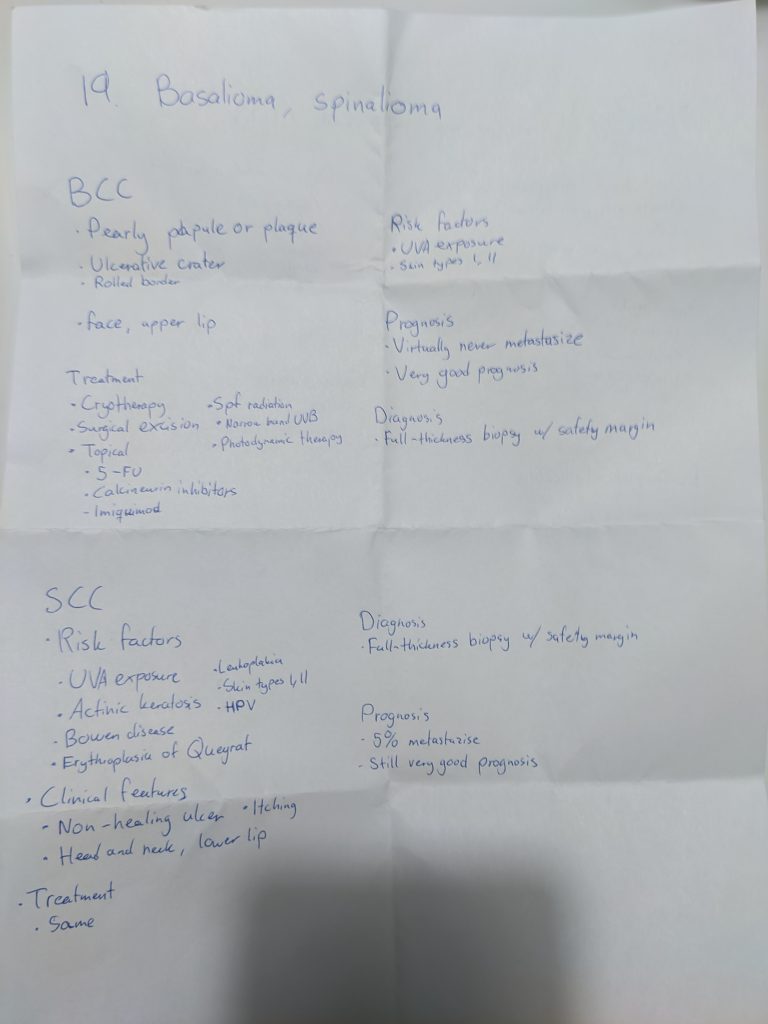
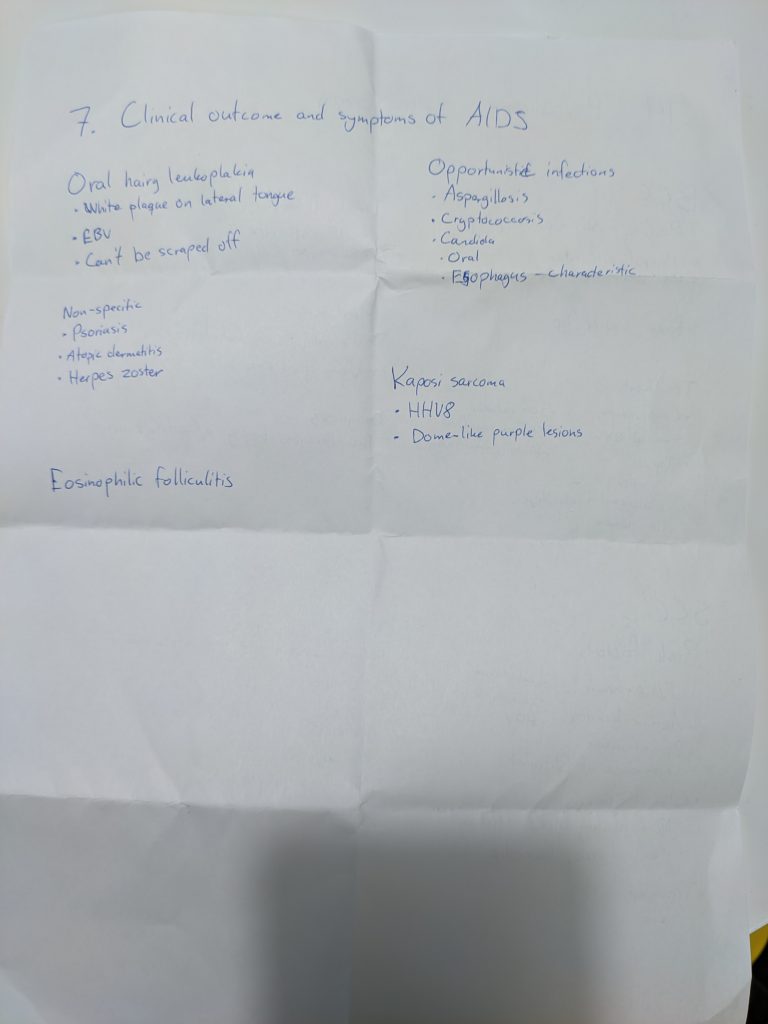
The A topic card I drew said “19. Basalioma, spinalioma”. “What the hell is this?”, I think. I was pretty sure that basalioma is another word for BCC, and I guess spinalioma could mean SCC, but I’m certain that that topic isn’t topic 19, so I’m super confused. Ágnes sees my reaction and explains that yes, these are BCC and SCC. Okay, fine, not a bad topic. My B topic was ” 7. Clinical outcome and symptomes of AIDS”. I say “shit, this sucks”, to which Ágnes replies “No, I think this is a good topic”. Okay, at least I know a few things here, I think to myself.
I sit down and prepare, and I write a good amount on the A topic, and a few things on the B topic. Definitely enough to get a 2 at least, also considering the people before me’s exams (we were preparing the same room as people were examined). It was true, Ágnes was VERY nice.
Eventually, the professor comes into the room. He says something to Ágnes in hungarian, she says something back and points to the remaining 3 or 4 students in the room. The professor says okay and then leaves. In my mind, the conversation went like “Are there many students left?” “No, only these few. I can probably examine them.” “Okay”. The professor is probably a busy man, he doesn’t want to waste time examining a few students.
Eventually, it’s my turn.
As I sit down next to Ágnes, she says “Just wait one minute, let me get the professor”. What? They’re changing examiner now? I start to get stressed, I know it’s always the department heads who take their subject way too seriously. But, I can’t really do anything else but try. He comes in and sits down. He doesn’t appear to be in a very good mood.
I start with the risk factors for BCC.
He’s already sighing, holding the bridge of his nose and taking long pauses. I can sense that he’s getting frustrated already.
That does seem familiar to me, but I’d never had remembered that. He takes another long pause, annoyed. I can sense the atmosphere in the room is super tense, as the other students in the room are following my exam closely, in horror.
– Another long pause –
I can tell that this is going to hell.
He sighs as if I didn’t know that. Of course it occurs on sun-exposed skin, wasn’t that obvious when I said that it’s related to UV exposure?
He sighs loudly, obviously annoyed by my answer.
That’s a valid point, of course, but are there any types of phototherapy that don’t use UV light? Not that I know of. Maybe the cancer is caused by UVB then, and using UVA is the answer.
He’s obviously annoyed, because in his mind I obviously didn’t understand what he just said. I realize that there is one last type of phototherapy I haven’t mentioned, so maybe that works without UV light and is the correct answer?
He laughs a little at my response.
For some reason, and in retrospect I realize that it was stupid to think that way, but I think at the moment that he’s after a therapy that I haven’t mentioned yet; that I still haven’t mentioned the main treatment. Now, I had already listed most treatment options I had written down, so I was running out of options. There was one of the topical treatments I hadn’t mentioned yet, so I went with that one. I think it was imiquimod.
His annoyance with me peaks. He shakes his head, sighs multiple times.
I don’t really know what to say to him. It’s obvious in retrospect that they’d rather remove the tumor than apply topical treatment. I think my wrong answer was partly due to me being very tired and not thinking clearly, and partly because I was certain that he was after something which I hadn’t mentioned yet.
As I get up and walk to pick up my stuff I get eye contact with the other students in the room, who were stunned. I could tell that the other students were scared now. I don’t think anyone expected him to be so strict, especially after the previous examiner. Luckily, the girl after me passed, but she told me later that it was barely and that it was a very bad experience. I don’t know about the others, but I hoped they passed.
It’s kind of ironic how I would probably have passed if I was one of the first students to go in rather than to stay outside and study more.
So that’s the story of how I failed derma. I haven’t failed an exam since the spring exam period of 2017, when I failed immuno after only studying 2 days for it (this was before I made notes). It was kind of a sobering experience, as I didn’t really expect to fail any exams anymore, especially after I was done with pathology and pharmacology.
It was surprising to have an exam in good old fashioned anatomy department-style©, where if you say the wrong thing once they’ll take it as if you don’t know the answer at all.
Anyone can fail at POTE; it happens to the best of us. I’m not immune to it either, despite being “greek doctor”.
The next possibility to have derma is next friday. I bought a ticket home to Norway for tuesday two days ago. I don’t want to lose that ticket and to have to stick around here for another week just for fuckin derma. I can take it next year as exam course without losing a year, so I’ll do that instead. I’m tired.
I’m not sad that I failed. I would be if I had to pass it this semester to not lose a year. I already started my vacay, although with a bit of a bad conscience.
Don’t be scared of derma because of my experience – I’m one of the very few I know who have failed it. For that matter, don’t be scared of ENT either – appearently nobody else (except one) had the same experience with the exam as I did. Maybe I just bring out the worst in department heads on exams?
I’ll write another post next weekend with some statistics and stuff. Good luck with your exams if you still have, and congratulations to those that are done already (although they probably won’t see this).