Password-protected images
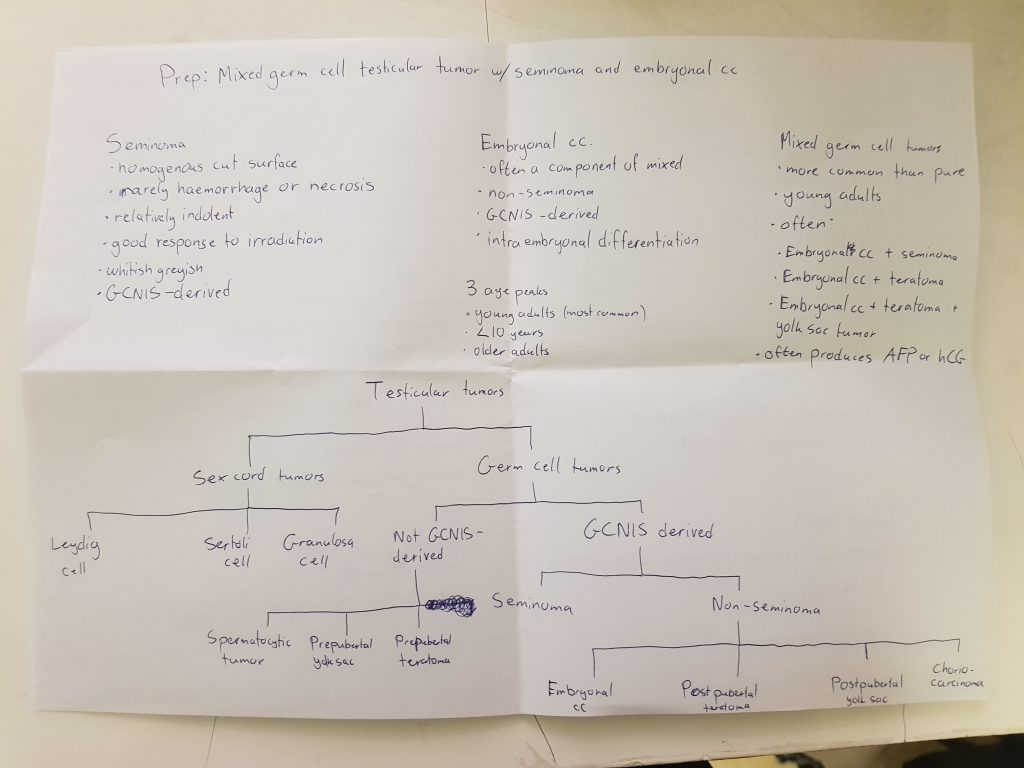
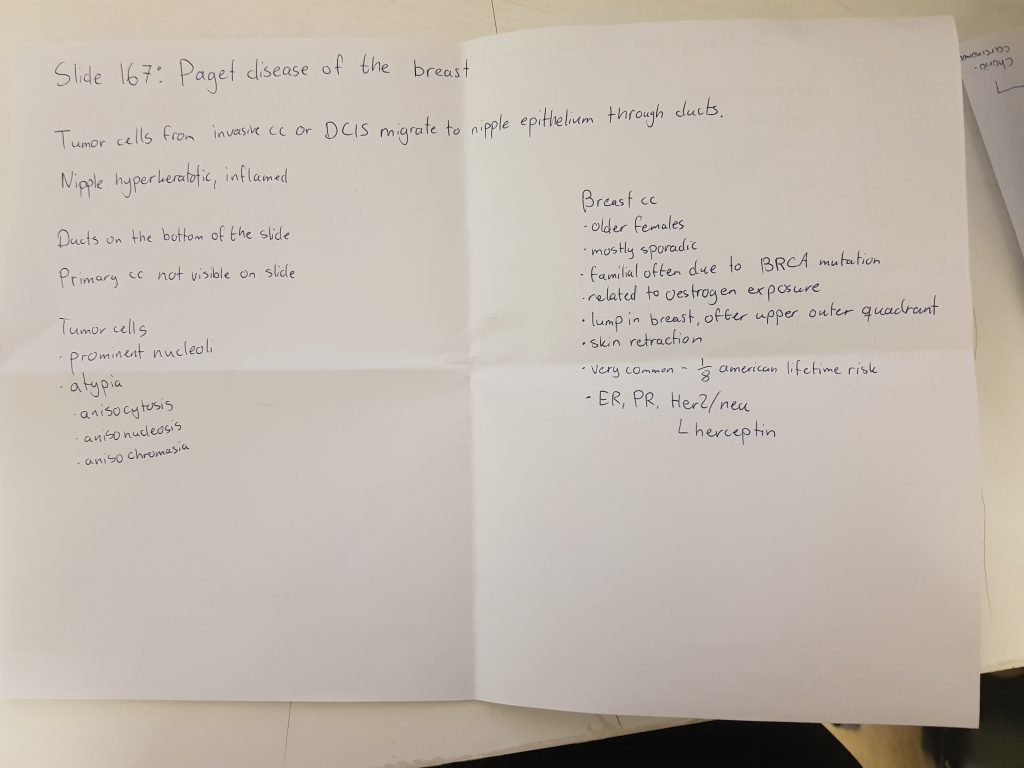
Some images are supplied by the departments at the university with the intention that they should only be shared among students. Because of this will I from now on password-protect these images. At the time of writing does it just include pictures of preparations and histopathology slides in pathology 1, and I’ll definitely do the same for pathology 2. This password-protection may extend to other subjects later, or I might even remove it if it turns out that the department doesn’t mind.
Why do I lock just the images? I believe knowledge should be freely available, so locking just the images with a password and keeping the text available makes more sense than locking the whole website with a password or any other solution.
There is only one password for the whole website. After entering it once will your browser remember the password for 30 days, after which you must enter it again. If you enter the password into one page will all other pages be unlocked, so you don’t have to unlock every single page.
If you’re a student at POTE can you send me an e-mail to get the password. I’ll also post it on Jodel so local students can find it easily. If you receive the password then please share it with fellow students. I apologize for the inconvenience caused by this, but I hope that it will come to a time where the password is spread by word of mouth so the process isn’t so inconvenient. I can see that by the time I applied the passord to the time of writing this (around one hour) has the password already been spread to some extent, which is great.
If you immediately recognize the origin of the password are you a star in my eyes!
Statistics
I thought people might be interested in seeing some website statistics for greek.doctor, so here goes.
There have been 9500 visitors since the exam period started December 10th. That’s an average of 250 students every day. The number of daily visitors was high from the 10th until the 21st, when number was 150-200 visitors per day. Good to see that people took some time off for Christmas despite it being in the middle of the exam period. January 2nd was the average back up to around 300, where it has stayed since.
During the same time period have there been 122 000 page hits, meaning that the average visitor only visits 12 pages, however I think this number is actually higher than that because I suspect that many “visitors” are just robots that only visit one page and not actual students.
There have been 22 500 visitors and 214 000 page visits since I started measuring statistics in June 2018.
The record for most pages visited by one person in a day is 278. On December 13th did one student in Hungary visit 278 pages on greek.
The day with fewest visitors is December 22th, closely followed by December 23rd. 151 and 185 visitors visited those two days, respectively.
The vast majority of visitors are in Hungary, but there is a considerable amount of visitors from USA, Germany and Norway as well, in that order.
The most popular subject by far is pathology 1.
There are 405 different pages in total. That’s a lot!
There are around 20-30 people every day that reach greek.doctor by search engines, mostly from Google but some also from Bing.
Most people that are referred to greek.doctor come from Google. In second place do we have Facebook, which is probably because people send each other links on Facebook messenger. Funnily enough are there also some referrals from Instagram, meaning that people either share links via Instagram chat or people actually click the link I have in my Instagram profile, which is flattering.
Lastly, if anyone have any privacy concerns: I have no way of identifying who visits the website. I can’t even see your IP address. The only information I can see from visitors is:
- How much time you spend here
- Which pages you view
- Which browser you use
- Which operating system you use
- Which country you are browsing from
- How you were referred here (i.e. I can see that many are referred here from Facebook)
- If you googled something to end up here can I see what your search word was.
Some thanks
I want to thank Sofia Akhtari (username “ms. worldwide”) for helping me write many of the theoretical topics in pathology 1 and pathophysiology 1. It really helped me a lot because there really is a lot to write!
I’d also like to thank all of you who comment to help me find inaccuracies and things I’ve gotten wrong and to improve the notes. Many people, but anonymous and pseudo-anonymous (looking at you, Johannes) have left many comments with improvements, and we’ve had some discussions as well. I really appreciate it!
What’s next?
I’m done for this exam period. Without making any promises or legally binding contracts can I say that I will try to write physiology 1 notes. They definitely won’t be finished before this exam period finishes, but hopefully will they be finished before the physiology 2 exam this spring, or possibly before the next autumn exam period. Don’t rely on it however, as I might not have time to complete them.
We’ll definitely write pathology 2, pathophysiology 2 and pharma 2 for the next semester. I probably won’t have time to write anything else.
If you still have exams left, good luck on them! If you’re already done, enjoy the vacation!
{kind=link}