Had radio yesterday. It took place in the large lecture room at 400 bed, where the blood transfusion lectures were. The exam lasted 1,5 hours or something. There were also Hungarian and German students there, so it was packed. There are multiple different tests, so you neighbour doesn’t have the same questions as you.
Around 20 out of the 100 questions were questions related to images. The images were continously cycling on the projector, but they were also in the exam paper booklet thing, so you weren’t dependent on the projector. The questions were organized like this:
Simple choice related to radiology
Simple choice related to nuclear medicine
Multiple choice related to radiology
Multiple choice related to nuclear medicine
Relationship analysis related to radiology
Relationship analysis related to nuclear medicine
Like 2 true/false questions related to radiology
Images related to radiology
Images related to nuclear medicine
There were far more questions related to radiology than to nuclear medicine, but still a considerable amount of nuclear stuff.
The images were of relatively basic pathologies, like hydropneumothorax on CT, ascites on ultrasound, epidural haemorrhage on CT, etc. Although there was one nuclear medicine image which tricked everyone. It looked like kidney scintigraphy at first glance but it was actually bone scintigraphy of the femur or something.
I didn’t think it was too difficult, but then again I studied 6 days and wrote notes, so keep that in mind. However, most people I know passed with only a few days of studying. I counted the questions I was 100% certain of during the exam, which were 64. Although I later found out that at least one of those were wrong (I though it was kidney scintigraphy), so there you go.
We got the grade at 14:30 the same day, which was nice. I got a 4, which is good of course, but I actually like radiology and studied a lot for this, so I actually wanted the 5. But I didn’t know the answer to many of the questions, so I didn’t deserve it anyway.
I remember some of the questions which I didn’t know the answer to, so I’ll go back to the notes and add answers to those to the notes.
I’ve noticed that I can’t study a subject without writing at least some short notes about the subject. So I thought I might as well upload them too. They’re under “other subjects”. As I write radiology this week I’ll upload it there too.
Had ENT yesterday. I studied 4 days of it, but those days included new years, so it was more like 3 days of effective studying. It has multiple practial parts and one theroretical part. There are separate examiners for the practical and theoretical parts. We waited at the entrance of the department until a teacher called us in 15 minutes later.
Practical parts
They took 2 and 2 students in to an examination room in the ambulatory unit. They brought in a healthy-looking patient for the examination. There are two doctors in the room, both are young doctors, one male and one female. The male was our primary examiner for the practical part, the female was the co-examiner.
The primary examiner takes out a bowl containing many instruments related to ENT. “Let’s talk about myringotomy”, he tells me. He asks me many questions, like:
In which quadrants can we perform myringotomy?
What are the indications for myringotomy?
He also takes out a myringotome and a grommet (it’s very small and comes in a blue box), and asks me what they’re used for. I mess up a lot on this part, mixing serous and suppurative otitis media and stuff. He still gives me a 4 at this part.
Next, he asks me to examine the patient’s neck. I start by palpating the retroauricular and preauricular lymph nodes, and I continue palpating the other lymph nodes, before he stops me and asks the names of the different lymph node regions, and which cancers drain into which regions. He also asked me the borders of the posterior triangle.
I make a lot of mistakes here, especially regarding the cancers. I call regions II, III and IV the upper, middle and lower internal jugular chains (which multiple other sources call them..), but he says that they’re called the parajugular regions. He gives me a 3/4 here. I never got to finish the neck examination, and I never examined the patient with a headlight.
Theoretical part
The theoretical part begins by you having to write down the top ten. I write down 9, but of course I forget the last. The male examiner from before takes my paper and looks at it, before he asks “What about hoarseness?”, and I suddenly remember the last one (the 3 weeks hoarseness one).
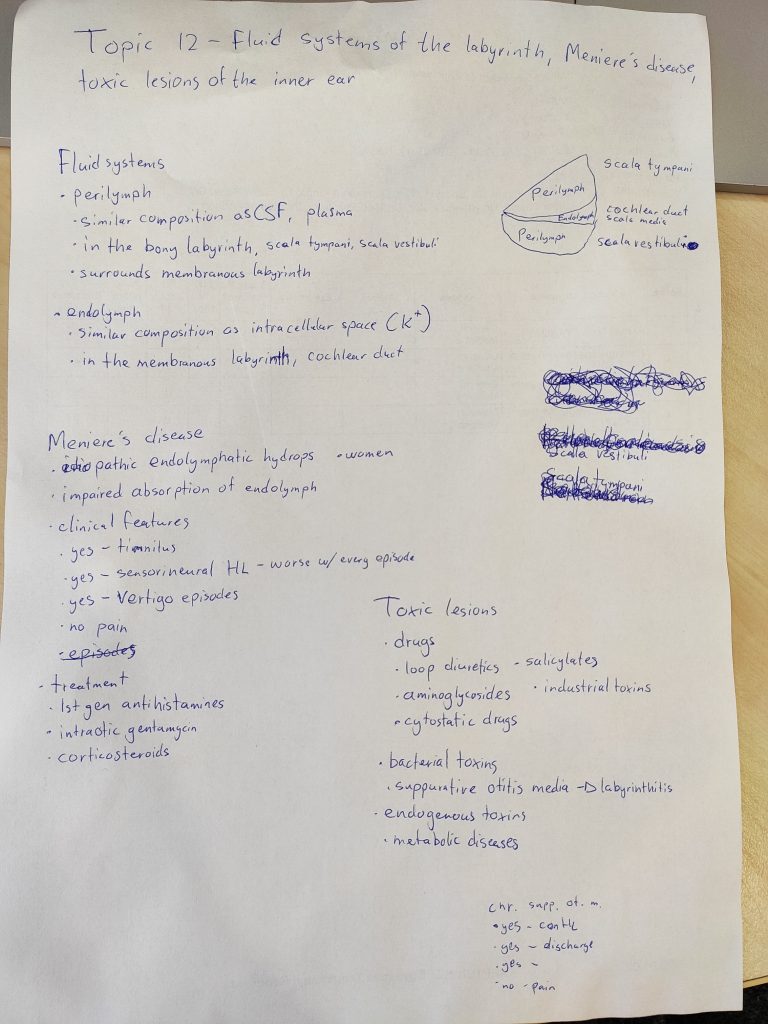
I’m then taken into an office, where I draw a topic and sit down to prepare. My topic was “Fluid systems of the inner ear, Meniere’s disease and toxic lesions of the inner ear”. Ps: the topics were in order, so that
After some preparation the man himself comes in. I start with my topic, explaining what I had written down about the endolymph and perilymph (not mentioning the drawing on the right, because I wasn’t totally sure about it). He has no questions there, so we move on to Meniere’s.
I explain what I had written down (I had the “no” wrong, I just noticed. He didn’t comment that). He asks me how to diagnose it. I tell him that you need a certain number of attacks within a certain time-frame, but I don’t remember the specifics. He asks me about other potential treatments. I don’t know any more, I tell him. That brings out the asshole in him.
“When you study a disease, do you just read about the symptoms and the pathophysiology and skip the diagnosis and treatment? If a patient comes in with this disease, they’re not interested in the pathophysiology, they’re interested in how you can treat them. What are you going to tell your patient when you don’t know how to treat them?
“How long did you study for this?”
“Where did you study from?” “The Thieme book” “Are you telling me that the book doesn’t write about the diagnosis and treatment of Meniere’s disease?”
“Everyone with this topic just mentions the three yes and one no and thinks that’s everything which is important”
I wish I told him to fuck off there and then, but that’s easy to say in retrospect I guess. Like, bitch, nobody retains everything they read, and if there’s something I don’t know as a doctor I would just look it up anyway. He was rude to the other students as well.
We move on to the toxic lesions. I mention what I had written down. He asks me for examples of metabolic diseases which can damage the inner ear. I didn’t know any examples so I guessed diabetes (always a good guess), which was appearently correct. He also mentioned uraemia.
He then asks me what the “three yes and one no” of chronic suppurative otitis media are. I remembered only two yes and one no (I forgot the perforated tympanic membrane), but when he asks “what causes there to be otorrhoea?” I remember the last yes.
He then asks me the four major symptoms of chronic rhinosinusitis. I spend some time thinking, and I recall three of them. “You forgot the most important one” he says, at which point I remember “nasal airway obstruction”.
He gives me a 3 in total, further dissing me for “skipping” the diagnosis and treatment when studying.
My tips to you would be to know the pathophysiology, symptoms, diagnosis and treatment of each disease, and definitely know the “three yes one no” for Meniere and chronic suppurative otitis media, the four major symptoms of chronic rhinosinusitis and of course the top ten (you can’t draw topic if you don’t know them).
The younger examiners were very nice and helpful though, even though I was grilled by the male one. Both examiners were in the room when I was examining the patinent, and I think they would help out with the hungarian if that would be a problem.
Next
Next is radiology written the 10th. It will be the first exam this exam period where I have enough time to maybe take it a little bit easier, which I’m looking forward to.
So I had public health 5 yesterday. I studied 2 days for it. My examiner was dr. Katalin Szendi. She was very nice, as all examiners appearently are in 3rd and 4th year (hopefully 5th and 6th too). She was fair and passed everyone before me that day, even though every one of us said stupid things.
You draw 2 topics, one from each envelope. I don’t know how the topics are separated into the two envelopes, but some people drew two consecutive topics, so it’s not divided in the middle.
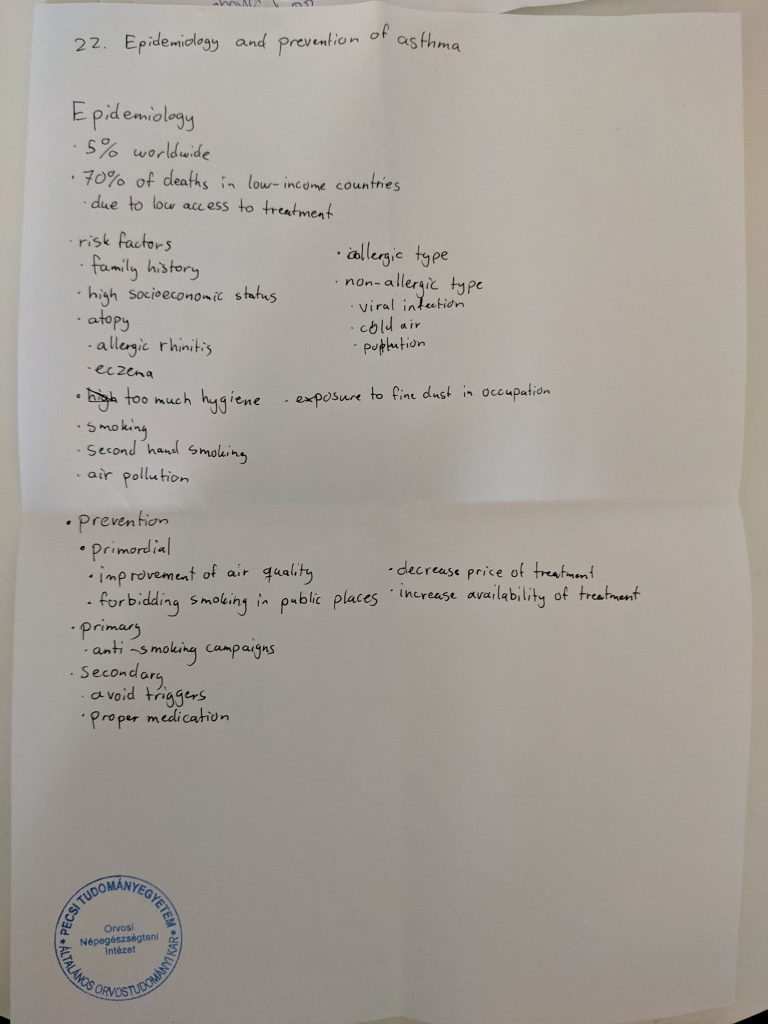
My topics were “16. Epidemiology and prevention of prostate and cervix cancer” and “22. Epidemiology and prevention of asthma”.
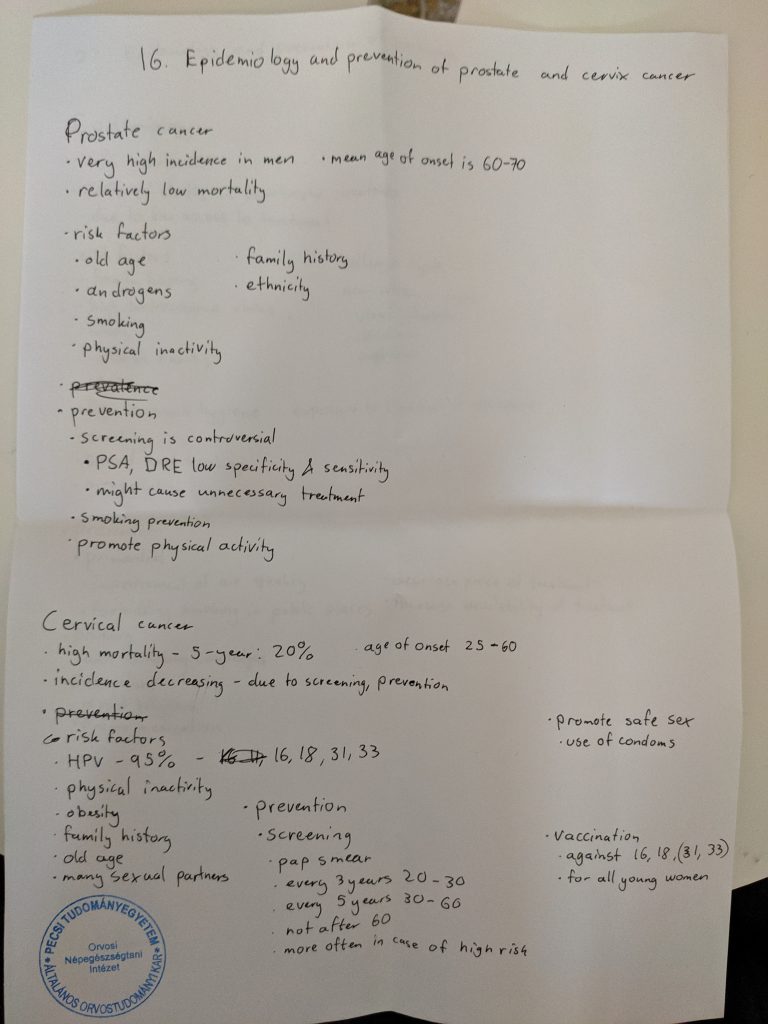
16. Epidemiology and prevention of prostate and cervix cancer
I began by explaining the incidence and mean age of onset of prostate cancer. I said that it has low mortality, to which she asked what the 5-year survival rate is. I said 30% (no idea why I said that), and she as like “but you said it has low mortality, 30% is not low”. I corrected myself, first to 50, then 70 and finally 80%, which is correct.
I mentioned the risk factors I had written down. She said that there is at least one more important risk factor related to lifestyle. I guessed diet, which is correct, but she wanted to know what part of the diet increases the risk for prostate cancer. I started to guess red meat, trans fats, saturated fats, salt, but that was not it. She says it’s a type of fatty acid. I started to guess all types of fatty acids I could think of, saturated, monounsaturated, trans fats, but no. I was pretty sure that polyunsaturated fats were not the cause, because they’re healthy, right?
Then she asks me what the remaining type of fatty acid is, to which I say polyunsaturated. She asks me what two types of polyunsaturated fats we have, and when she said that I remembered omega-6 fatty acids, which was correct. She told me to move on to cervical cancer.
I start by saying that the incidence is declining due to screening and prevention, and that the 5-year survival is 20%. I talk about the risk factors I had written down, and she says that there is another important risk factor. I suddenly recall that having many full-term births is a risk factor. She asks the mechanism behind this.
I didn’t know the answer, and I couldn’t think of anything. I came up with a really stupid guess, which in retrospect was obviously wrong. I don’t really know why I said it. Maybe I saw an opportunity to be funny?
“Because having many births is related to having lots of sex?”
The examiner starts laughing hysterically. The co-examiner starts laughing too. The other students in the room also laugh. I laugh at how I could say such a stupid thing.
After a minute straight of laughing, the examiner asks me what happens with the cervix during delivery. “It’s dilated”, I say. “What else?” “It’s physically injured?” “Yes, injury to the cervix makes it more susceptible to HPV infection.”
She asks about which genetic factors are involved. I say BRCA, to which she says yes, but that’s not the most important. I guess the androgen receptor. She says not really, but it has to do with androgens. I guess the 5-alpha reductase enzyme, and she says yes.
She asks about prevention. I mention what I had written down. She asks me what types of vaccines we have. I say that we have the bivalent against 16 and 18, and the quadrivalent against 16, 18, 31 and 33. She says that that’s not correct. I realize the mistake and say 6, 11, 16 and 18. We move on to the next topic.
22. Epidemiology and prevention of asthma
I basically read everything I had written down. She asks me about another primary preventative measure. I half-guess breastfeeding (because I remembered that it was protective against some immune-related diseases), which was correct. She asks me how long it’s recommended by the WHO to breastfeed a child. I guess 1 year, but she says 6 months.
I think she might have asked me one or two more questions but I can’t remember.
She ends up giving me a 4, and says that the dietary risk factors for prostate cancer were was prevented me from getting a 5.
Christmas break
That’s all the exams before christmas for me. I leave for Norway on sunday, and I return the 29th. Hopefully I can relax and recharge during my time at home, so I can be ready to tackle ENT the 3rd (I hate ENT).
I had Clinical Biochemistry yesterday. I studied 3 days for it. My main examiner was Dr. Tamás Nagy. Dr. Ágnes Péterfalvi was the co-examiner. The exam takes place in the department. We showed up outside where the clinical biochemistry seminars took place.
You draw two random topics from one pile. Few examiners give you a lab result to analyze; the examiners yesterday only gave them to those who were between two grades. Even then, they didn’t have to come up with a diagnosis based on the results. It was more of a discussion of what the result tells you, what differential diagnoses can be, what the next steps in diagnosis can be, etc.
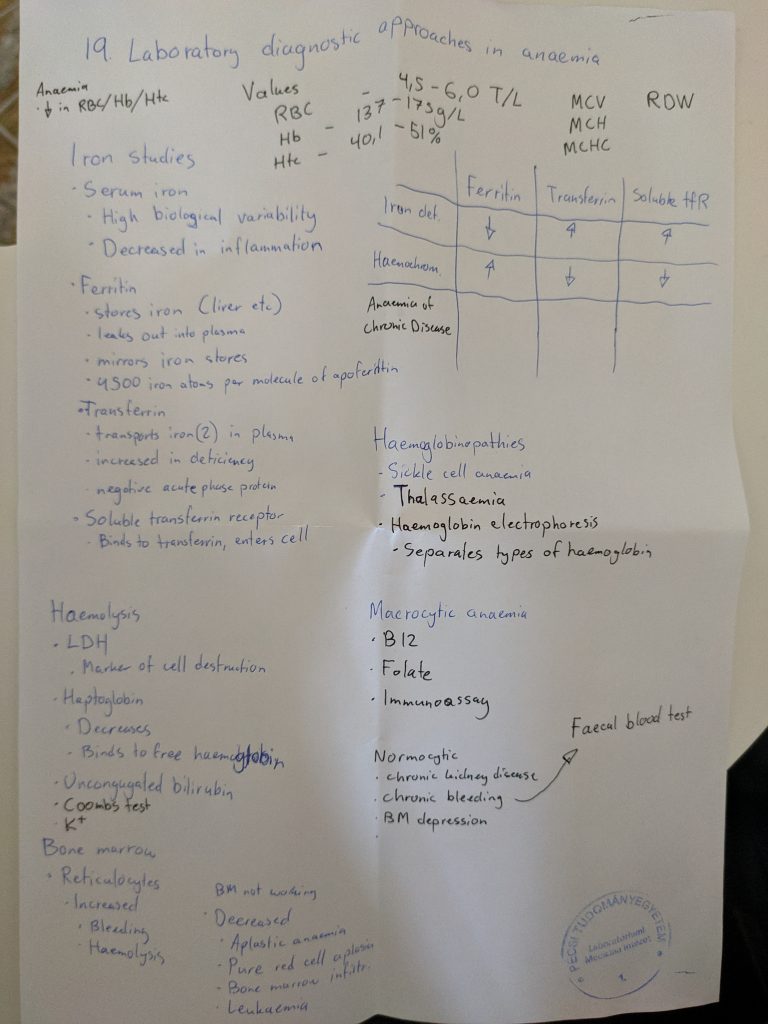
My two topics were “19. Laboratory diagnostic approaches in anemias” and “48. Tumor markers and their informational value in the clinical laboratory practice”. The subject and exam are plagued by typical POTE bullshit which I will explain more about later. There are some topics which are 0% covered in the lectures or seminars, like 27 (only like 2 slides with no useful information), 39 and 40.
19. Laboratory diagnostic approaches in anemias
This was my best topic. I had written down almost everything which is important. I began by saying that the definition of anaemia is a reduction in RBC count, haematocrit or haemoglobin. The examiner stopped me by saying that it’s wrong, and only the haemoglobin matters for the diagnosis of anaemia. What he said isn’t correct according to uptodate or even the co-examiner’s own seminar! She was my seminar teacher and I have her powerpoints. Typical POTE bullshit.
Anyway, I go on by talking about the classification according to cell size, what the different causes of microcytic, macrocytic, normocytic etc. can be. While I’m talking about haemolytic anaemias the examiner says “I think it’s appearent that you know this. Let’s go to the next topic.” Good start!
48. Tumor markers and their informational value in the clinical laboratory practice
I start by explaining the definition of tumor markers. I explain that they’re often low sensitivity and specificity and therefore not useful for screening or diagnosis. I say that they’re value lies in determining prognosis, monitoring treatment response and relapse.
I mention some examples of tumor markers, the ones I had written down. There’s not much more to say (there’s wasn’t much more on the lecture). They then start to ask me many questions about stuff which wasn’t on the lecture. I don’t know the answer to many of the questions. They try to help me with the answer to each question, in some cases I can think my way to the answer but in other cases I couldn’t.
They then decide to give me 4. I immediately get a little angry inside, because I had mentioned everything they taught us about tumor markers and that somehow wasn’t enough for a 5? What?
I ask them if I can fight for a 5. They accept. They ask me some questions (more questions about stuff which wasn’t on the lecture). They also give me a lab test to evaluate. They eventually agree to give me a 5, even though I didn’t really answer many of their questions, at least not without a lot of help.
I remember some of the questions from my exam, but to be honest I can’t remember which questions were asked before they wanted to give me a 4 and which ones they asked after I asked to fight for a 5. Anyway, here they are.
Tamás: Do you check the PSA before or after you do rectal digital examination?
Me: After?
T: No, you do it before. Why?
(No idea)
T: During rectal digital examination you might physically stimulate the tumor or benign prostate hyperplasia, which can stimulate them to release PSA, which gives a falsely elevated result.
T: Do you know a non-cancer factor which increases CEA?
(No idea)
T: It’s a bad habit many people have.
M: Alcohol?
T: No, the other common bad habit.
M: Smoking?
T: Yes, smoking can elevate CEA and cause a false positive result.
T: PSA can be elevated in both BPH and prostate cancer. What can the laboratory do to make the PSA measurement be more specific for cancer?
(No idea)
Turns out you can measure “free” PSA, and the free PSA is more specific for cancer. Lower free PSA means increased risk for cancer.
They gave me a lab test. The test includes reference ranges and exclamation marks at the tests which are outside the refence. The lab I saw had elevated CEA and CA 19-9, cholesterol, uric acid and a positive stool blood result.
T: What can this be?
M: Probably GI cancer, it explains the blood in the stool, and the tumor markers are often elevated in GI cancers. High cholesterol can also be a sign of bad diet, which is a risk factor for these cancers.
T: What can explain the elevated uric acid?
M: Maybe this test was taken after chemotherapy and it’s due to tumor lysis syndrome.
T: Yes, most likely.
They also asked me about K-RAS, what it is and why it’s important. I said it’s a proto-oncogene which can be mutated in GI cancers. They agreed and asked what the importance of it is. With some help I arrived at the conclusion that K-RAS can be tested for in cancers, and its mutations influences the prognosis and treatment of the patient.
Other than the typical POTE bullshit they were very nice. It was almost impossible to fail with them, so I wouldn’t worry about failing clinical biochem. I studied the lectures and seminars, and even though they appearently don’t contain all the information they expect us to know, it should be more than enough to pass. They also ask basic stuff from patho and pathophys, nothing difficult.
My next exam is public health on thursday. I was originally planning to do derma on friday, but I realized I’m way too tired to do that, so I changed it to public health instead.
So I had haematology yesterday. It’s a written exam, with simple choice and multiple choice questions. There are 40 questions on the test, each worth 2 points. You can get 20 points from the oral test, so the total max is 100 points. Some of the questions are based on cases. We were supposed to get our grade before 14:00 yesterday, but we got it this morning.
I had pharma on monday, so I didn’t have much time to study for it. Upper year students will tell you what material to study, and they’re not wrong; you should listen to them. However, of the 40 questions on the exam, I was only 100% sure about 10 of them (based on the previously mentioned material) while the remaining questions were difficult, so I wasn’t expecting anything else than a 1 or maybe 2. In the end I got a 4 somehow. Maybe the grades were normal distributed, or maybe the 30 questions weren’t as hard as I thought.
My tip to people studying for haema: definitely study what upper year students tell you to, but also focus on the treatment of the important malignancies, especially lymphomas, leukaemias and multiple myeloma. Learn the drugs and chemotherapy regimens used (just their names) and when stem cell transplant is used. Everyone I know who had pharma on monday and had haema yesterday passed it. You’ll be fine.
My next exam is clinical biochem on monday. Hope they’re nice.
So I had pharma 3 yesterday. My examiner was prof. Gábor Pozsgai and he was very nice. I got two topics I liked and one which was meh, but I was hoping to get the 5 this time. In the end he asked me many things I couldn’t answer, and so I got a deserved 4.
There were four examiners who examined yesterday. Prof. Pozsgai, prof. Pethő, prof. Barthó and dr. Bölcskei. Prof. Helyes and prof. Pintér were not present.
You draw three topics, one from each pharma semester. My topics were “Local anaesthetics”, “Laxatives, antidiarrhoeal agents, drug treatment of inflammatory bowel disease and paralytic ileus, digestives, drugs used in cholelithiasis” and “Antiviral drugs against herpes, hepatitis and influenza viruses”.
As you might notice, my pharma 3 topic included influenza viruses, which, according to the topic list in the course information, should belong to the HIV topic. They moved influenza drugs from the HIV topic to the herpes and hepatitis topic.
Drug walk
My first question was to define potency. I defined potency correctly, but when I messed up when defining the ED50. I said that the ED50 is the concentration which gives the desired effect in 50% of patients, which is wrong. He told me that it was wrong, I corrected it and it was fine.
Then he asked me the differences between first and second generation antihistamines. I said that the first generation ones penetrate the BBB more easily, causing more sedation, and that the first generation ones block muscarinic receptors to a larger degree, causing side effects like dry mouth and constipation.
Then he asked me which drugs could be used in congestive heart failure. I said ACE inhibitors, AT2 antagonists, beta blockers, calcium channel sensitizers, cardiac glycosides and diuretics. He asked me what the indications for cardiac glycosides would be, as they’re not first-line agents. I didn’t know, but he said that they’re used if the patient has another condition in addition to the heart failure. I remembered that glycosides are anti-arrhythmics (even though I forgot to include them in the anti-arrhythmic topic, whoops), and so I said that maybe they would be preferred if there was also an arrhythmia. He said yes and asked which arrhythmia. With a qualified guess I said atrial fibrillation, which was correct.
Then he asked me to list the types of antianxiety and hypnotic drugs. I mentioned benzo’s, barbiturates and z-drugs. He asked me for a drug which is an anxiolytic but has no hypnotic effect. I asked if he meant any antidepressants, but that’s not what he was after. I remember that there were some atypical anxiolytics mentioned at the end of the benzo topic, but I couldn’t remember the name or the mechanism. He helped me by saying that it acts in a different manner than the other anxiolytics, but in the end I couldn’t produce the answer. He said that he was after buspirone. To be honest I had that name in my head when I was trying to find the answer, but I wasn’t sure so I never said it. Just goes to show that you should trust your gut.
He then asked me about the types of oral antidiabetics which don’t carry a risk for hypoglycaemia. I said metformin, GLP-1 agonists, DPP-4 inhibitors, SGLT-2 inhibitors and glitazones (I forgot the alpha-glucosidase inhibitors). He asked me which ones increase the risk for urinary tract infections, and I said the SGLT-2 inhibs. He asked me if I could name any, but I was honest with him and told him that I have given up trying to remember the names of the oral antidiabetics. It was fine, and we moved on to topics. He asked me which topic I wanted to start with.
Local anaesthetics
I wrote the spinal side effect thing on the bottom during the exam, so I could remember that he asked that.
I didn’t present the topic, he started by asking questions.
Examiner: What is the mechanism of action of local anaesthetics?
Me: They block sodium channels from the inside of the cell. They must diffuse into the cell, so they’re lipophilic. Inside the cell they’re ion-trapped, because these drugs are bases. This block is use-dependent.
E: What does it mean that it’s use-dependent?
M: It means that these drugs preferentially block the more active sodium channels.
E: What are the mechanisms behind this?
M: The drugs physically block the opening of the channels, so the more often the channels are open the more opportunities the drug has to plug it.
E: Yes, and there’s one more mechanism.
(I didn’t know that)
E: It has to do with its conformation.
M: Do they stabilize the channels in their inactive conformation?
E: No, not really.
M: Then I don’t know.
E: Okay, what can you say about the pharmacokinetics of these drugs?
M: Their effect is terminated when they’re absorbed into the systemic circulation.
E: Yes. Can you mention some side effects?
M: Yes, they’re bases so they can cause histamine release (I don’t know if this is true actually). They’re also cardiotoxic, so they can cause arrhythmia and negative heart effects.
E: Not really arrhythmias, but negative heart effects, yes. There are some special side effects when they’re given as spinal anaesthesia.
M: I don’t know.
E: They’re really characteristic side effects.
M: I don’t know.
E: Okay. Can you mention some local anaesthetics?
M: Yeah (I listed the ones I had written down).
E: Which is more long-acting, tetracaine or procaine?
M: Tetracaine. (Pure guess)
E: Yes. Do you know anything special about bupivacaine?
M: Hmm, I remembered prof. Gregus talked about the treatment of its intoxication.
E: Yes, what was that?
M: So bupivacaine is cardiotoxic, and if it’s injected into a vessel by accident it can be fatal. It’s lipophilic. By giving a lipid formulation like intralipid intravenously the lipid formulation can “dissolve” bupivacaine out of the heart.
E: Yes, do you know the original use of intralipid?
M: Yes, it’s used for parenteral feeding.
E: Yes, next topic.
Laxatives, antidiarrhoeal agents, drug treatment of inflammatory bowel disease and paralytic ileus, digestives, drugs used in cholelithiasis
I wrote the biological treatment of IBD during the exam
M: Okay, so we have four types of laxatives. Bulk laxatives, osmotic laxatives, faecal softeners and stimulant laxatives.
We talked a bit about laxatives, I don’t remember exactly what was said. I remember some of his questions
E: What’s another use for lactulose?
M: It’s used to treat hepatic encephalopathy.
E: And how does that work?
M: It acidifies the lumen of the GI tract, protonating ammonia to ammonium, preventing it from being absorbed.
I forgot the non-absorbable salts as osmotic laxatives. He tried to make me remember them by giving me some hints, but I had forgotten that they existed. He also talked about a faecal softener which is not on greek doctor and which I had never heard about. He also asked about the pharmacokinetics of senna glycosides, which I knew nothing about. Do they even have any pharmacokinetics? I also forgot adsorbents as antidiarrhoeal agents, and mebeverine.
E: Can you give me the drugs used to treat IBD? (funny, I was asked the same thing in pharma 2, and I have Crohn’s, so. Ironic)
I listed the ones I had written down, but while reading them I realized that I had forgotten to write down the biological treatment, but I remembed their name.
E: Which disease is the biological drugs more important in?
M: Crohn’s. (I’m actually going to start adalimumab in a few weeks)
He didn’t ask me anything else in this topic.
Antiviral drugs against herpes, hepatitis and influenza viruses
Notice how I messed up by forgetting gancyclovir, valgancyclovir and for saying that penciclovir and famciclovir are activated by UL97 kinase. I also forgot ribavirin when listing hep C drugs. I remembered it during the exam, but wrote it under the wrong hepatitis.
I began by listing drugs against herpes viruses. He asked about the mechanism of action of foscarnet. He asked me why we need prodrugs for these antivirals. Then he asked me about antivirals to treat EBV, or so I heard. I’m pretty sure I heard EBV, but I might have heard wrong, or he might have said wrong, because I’m pretty sure he was after ganciclovir and valganciclovir, which are used to treat CMV, not EBV. He asked me how antivirals are specific against virally infected cells.
E: What are the side effects of these drugs?
M: CNS toxicity? Hepatotoxicity?
E: No.
M: Nephrotoxicity?
E: Yes. How are these antivirals metabolized?
(I was pretty sure that they’re not metabolized but rather excreted renally unchanged. But I also didn’t think that he’d ask me a trick question like that, so I started guessing)
M: Are they metabolized by xanthine oxidase?
E: No, they don’t resemble nucleosides enough for that.
M: Then I don’t know.
E: They’re not metabolized, they’re excreted renally.
M: (jesus) So it was a trick question?
E: Yes (said with a stone cold face)
Then we went on to the hepatitis B drugs. He started by asking which hepatitises can be treated pharmacologically. I said B and C. I then listed the drugs I had written down.
E: What is the other use of these drugs?
M: Against HIV.
E: Yes. What’s different in the treatment of hep B and C?
M: The treatment of acute hepatitis C is curative.
E: Yes.
We went on to hepatitis C. I listed the drugs.
E: There is another drug which is very old, but still used. It might’ve been mentioned in other topics but it’s also used to treat hep C.
M: I don’t really know.
E: It causes some haematological side effects.
M: Ribavirin?
E: Yes.
He might have asked me some other questions about hep B and C, but I can’t remember now. We went on to influenza drugs.
M: Amantidine is used in influenza A. It inhibits an ion channel called M2, which is important for viral replication.
E: Can you be more precise about the step in the replication the M2 channel is important for?
M: No, not really. I don’t know.
E: Okay, continue.
M: We have oseltamivir, used for both influenza A and B. It inhibits neuraminidase, which is necessary for the release of the virus out of the cell.
E: Yes.
M: There is also baloxavir marboxil, which inhibits cap-endonuclease or something.
E: I’ve never heard of this drug.
M: Oh, haha. It was talked about in the seminar. It’s very recent I think.
E: Okay. There is a drug which has similar action to oseltamivir but has a very special way of administration.
M: Oh yeah. It starts with z, I don’t remember the name. It’s given by inhalation
E: I wouldn’t really say that it’s inhaled.
M: What? Then I don’t know.
E: It’s given by nasal spray.
It doesn’t say that on the seminar or in the book. It says that it’s given as a powder for oral inhalation, so he was definitely wrong about that.
And that was that. He spent a long time examining (especially compared to other examiners), but he was very nice.
Next
I have haematology on thursday and clinical biochem on monday.
I think greek.doctor is nearing its end. There aren’t any more subjects I want to write notes for, and I’m very, very tired of doing this. It takes a lot of time and energy, maybe more than most people think. Right now there are 817 pages, only maybe 10 of which aren’t topics and the vast majority of which I’ve written myself (the rest are written by my girlfriend, Sofia (msworldwide)). Almost all of these 817 pages are multiple pages long documents, and I spend maybe 2-3 hours per topic on average. I’ve been giving myself a lot of work by doing this, and I’m very glad that I did (maybe except for hema), but now I need time for myself to work on my mental health and engage in my hobbies.
I won’t take down the website. I’ll keep it up until it’s no longer used, which could be never. I’ll continue to maintain it by answering comments and fixing errors. I’ll post some statistics at the end of the exam period, as people seem to like that, and I think we’ll break the record again (like we do every exam period).
Oh, and by the way, I’ve made less than 5 euro from the advertisement on the page. I’ll keep it until the end of the exam period, but I’ll probably remove it as it’s not really worth having.
For the physiology 1 notes I won’t add the individual topic to the menu on the sidebar. Please give me feedback on whether you miss the sidebar menu for these topics or not.
Also, can anyone tell me which topics are included in the physiology midterm and when it is?
So I had pharma 2 yesterday. My examiner was Dr. Kata Bölcskei, and she was extremely nice. My topics were “Anticoagulants and antiplatelets” and “Psychomotor stimulants and nootropic agents”. You draw two topics, one from each of two piles. The first pile contains topics 1 – 15, while the second pile contains topics 16 – 34.
I performed really poorly today, so thank god Kata is super nice. I hadn’t eaten today and I was tired, so I couldn’t really focus, neither when writing my topics or when answering her questions.
Drug walk
She started with the drug walk with all students. They consisted of three simple questions. Mine were:
Can you mention some preferential COX2 inhibitors?
Can you mention some drugs that are used to treat IBD?
Can you explain the mechanism of action of cardiac glycosides?
For the first question I didn’t quite catch that she said preferential and not selective, so I said celecoxib. I thought celecoxib was selective, but luckily for me it’s actually preferential, so she accepted it. And then I said “the other coxibs”, because I couldn’t remember the names, but then she said that they are selective and not preferential, and that’s when I understood that she wanted the preferential ones. I hadn’t really learned which are preferential and which are selective, so the only other one I knew was paracetamol. She wanted me to say one more, but I didn’t know. She was like “it starts with M.. melox..” but I couldn’t finish it because I had totally skipped that. It was meloxicam.
I was really glad when I got the second question, because I have Crohn’s and should know that. I still managed to forget one of the most important drugs, azathioprine, which I’ve even used myself… I listed corticosteroids, methotrexate, cyclosporin (not really used), rituximab (not really used), infliximab and adalimumab. I then said “the locally acting aspirins”, and then she asked me what the active compound of these drugs are. I answered acetylsalicylic acid, but she was like “but that’s aspirin. These are not aspirin. It’s not acetyl, it’s another chemical group that starts with A”. With that hint I managed to guess that it is aminosalicylic acid. I’ll have to correct that in the notes.
For the last question, I said that they inhibit the sodium potassium ATPase, causing more sodium to remain in the cell, which causes calcium influx which stimulates contractility.
That was the end of my drug walk. Other people were asked questions like “could you list me some synthetic/semisynthetic opioids, could you list me some serotonin agonists” and stuff like that.
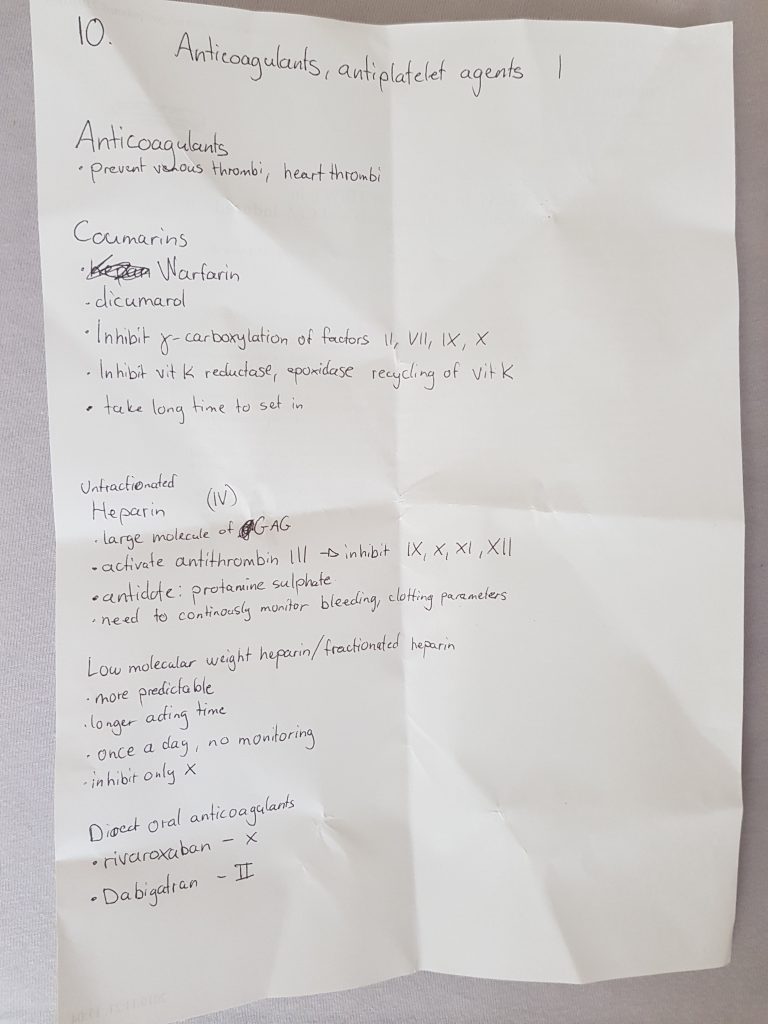
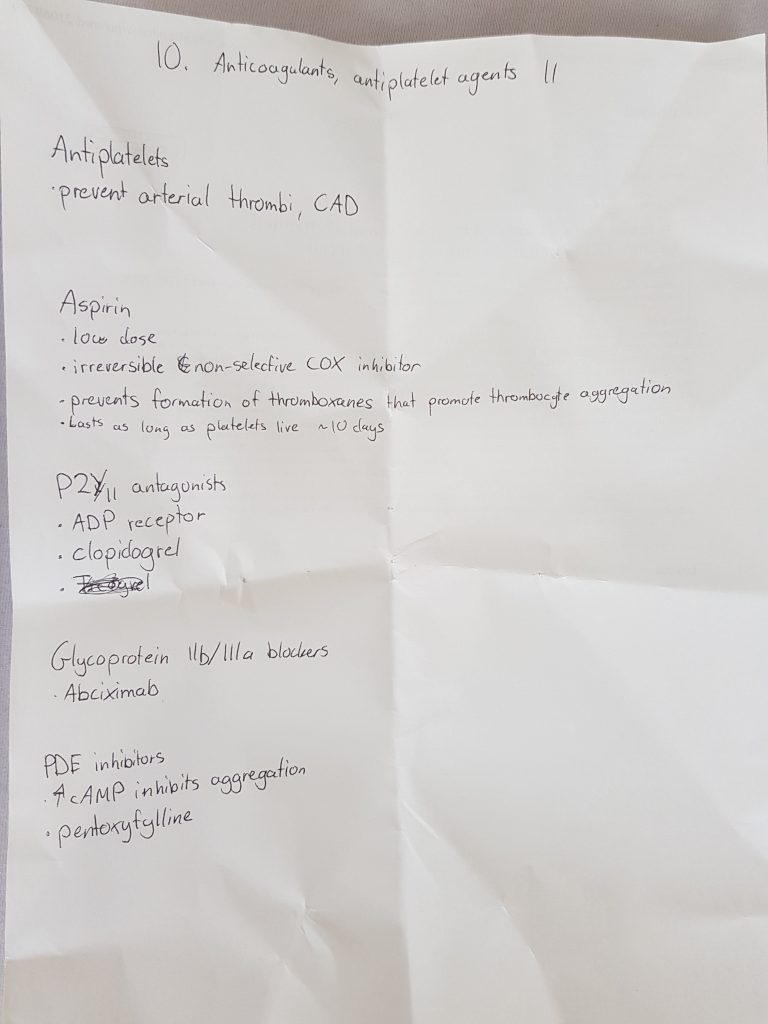
Anticoagulants, antiplatelets
She begun by telling me that I don’t need to talk about antiplatelets, only anticoagulants, which was kind of weird and it sucked because I knew more about the antiplatelets than the anticoagulants. It might have been a blessing in disguise though, because I mixed up pentoxyfylline with dipyridamole.
I began by saying what I had written until I was done talking about coumarins. Then she started to ask me questions that I 100% definitely should know, but didn’t. It went like this:
Kata: “How long does it take for warfarins to be effective?”
Me: “One week”
K: “No, it’s just a couple of days. How do you administer warfarins?”
Me: “IV”
K: “That would only make sense if they were not orally absorbed, which they are. What else can you tell me about the distribution, elimination.”
After some help I remembered that they have high plasma protein binding, and that they’re eliminated by biotransformation.
K: “Yes. Which enzymes are involved in the biotransformation?”
At this point I was trying to remember which CYP enzyme it was, but I ended up just saying CYP enzymes and that was fine. She didn’t want the exact enzyme.
K: “What would happen to a patient if they were on warfarin but also on other drugs like valproate, or something” (She mentioned other drugs as well, don’t remember which ones.)
I caught on that we were talking about drugs that are CYP inducers, so I said that the warfarins would have decreased effect as they would be metabolised more quickly.
K: “And what would happen if a patient on warfarin one day for example ate a lot of vegetables”
Me: “They might consume more vitamin K and therefore decrease the effect of the warfarins”.
K: “Which parameters should be monitored for warfarin?”
I answered prothrombin time, which is correct but she said that the prothrombin time differs between laboratories because they use different methods, so we use a standardized measurement. I couldn’t remember it but of course the answer is INR. I couldn’t even remember what it stands for.
K: “How much should the INR be?”
I said 1.5, but it’s actually around 2.5 – 3.5
Then we finally started to talk about heparins. I said what I had written, and then she asked questions. She asked “So what is the route of administration for heparins?”. I said IV, which is true, but she wanted me to say subcutaneous as well (which I didn’t). I then talked about the LMWHs. She wanted me to mention specific names, but I couldn’t remember any. She tried to help me remember them by saying that they end in -parin, but I didn’t really remember them anyways.
She asked me what the rare adverse effect of heparins is, and I remembered heparin-induced thrombocytopaenia. She asked me what the treatment for this is. I answered fibrinolytics but appearently there are thrombin inhibitors that are given for this. I think the name was lepirudin, because she said it was a protein found in the saliva of leeches, but that drug isn’t mentioned on the lecture so idk.
Finally we moved on to psychomotor stimulants.
Yeah, I got the PDE inhibitor name wrong. At least pentoxyfilline is also a PDE inhibitor
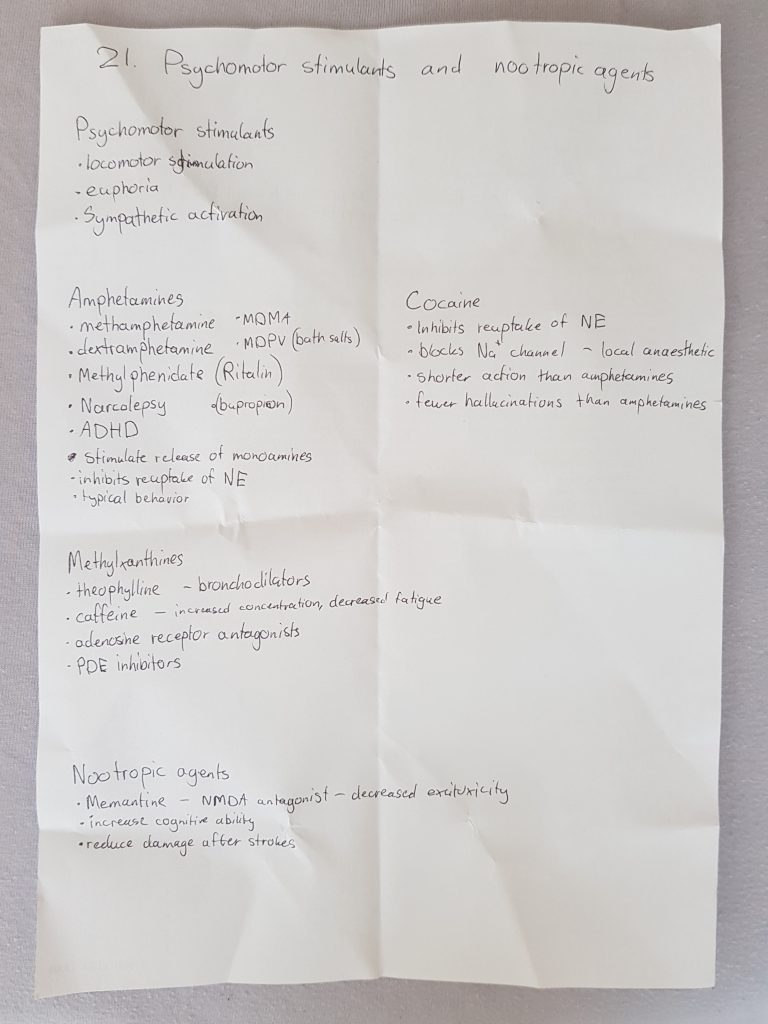
Psychomotor stimulants
I began by reading what I had written down about amphetamines. She then asked me about the dangers of intoxication of amphetamines, which I hadn’t written down because I thought that was part of the drug abuse topics. I said stuff like excessive sympathetic activation, psychosis, potentially water intoxication, but I forgot hyperthermia.
I then proceeded with cocaine, saying what I had written down. She then asked me whether the effects of cocaine are similar or different than those of amphetamines, and I said they’re similar. She said that cocaine is also used as a topical vasoconstrictor during bleedings or something.
Then I said what I had written about the methylxanthines. She didn’t really ask me anything there.
Then she asked about dependence of psychomotor stimulants. I said that dependence is mostly psychological.
Finally we arrived at nootropic drugs. I explained what they are and what they are used for, and I mentioned the only example I remembered (memantine) and how it works. She asked me about other nootropic drugs, but I couldn’t remember any. She tried hard to help me remember them, by giving me the first letter or saying that the brand name is “Nootropil” and stuff. She said that some vinca alkaloids are used as nootropics, but I couldn’t remember the name.
After this she said that my anticoagulant topic was okay, but she had to help me a lot to remember stuff (she even said that other examiners might not have been as patient as she was..). The psychomotor stimulants was not so good, she said. She wanted to ask me more questions to get a 4.
She asked me if I could explain some mechanisms of action of antiepileptic drugs. I began with the most common one, the use-dependent inhibition of sodium channels. She wanted me to mention some drugs that use this mechanism. I said phenytoin and gabapentin, but she stopped me and said that gabapentin uses another mechanism. I said that gabapentin blocks calcium channels.
She asked for some antiepileptics whose mechanism of action involves GABA. I didn’t remember their names. She tried to help me remember by saying that they have “gaba” in their name, but I still couldn’t remember. She said that they are not so important anyway.
She asked about a newer antiepileptic drug which has much less side effects than others. I didn’t know, but I think the answer was lamotrigine.
She asked me to talk about the “Z-drugs”. I explained their mechanism and indications, and I mentioned zopiklon but forgot the name of zolpidem.
That was the end of it. She said that I should be able to produce more information on my own, without needing help to remember.
Closing thought about the exam
I got the 4 in the end, but to be honest I performed worse than I was expecting from myself so I don’t really feel that I deserve it.
I listened to exams before me, and trust me, you can get away with lacking knowledge about A LOT (like what sildenafil is..).
I know many are scared of the pharma 2 exam, and it’s probably mostly because it’s most people’s first oral pharmacology exam, so we don’t really know how the exam will be. I don’t know whether it’s possible to observe pharma exams like in anatomy, but if it is, maybe observing some exams can help you realize that they don’t require significant knowledge from your part. They mostly ask basic stuff, and even if you forget or don’t know some things, it’s perfectly fine. I know it may seem like my experience with Kata might not reflect how other examiners are, but I’ve heard that most examiners are very nice. I also think that Kata and Dr. Gábor Pozsgai examine most international students, and they’re both very nice.
Some statistics
Appearently people liked the statistics post from last semester, so I’ll do it again. I know it’s not the end of the exam period yet and there will probably be more statistics during week 7, but if I make this post after the exam period is finished no one will find it.
The peak on January the 7th is actually due to a robot spamming thousands of views on the hypertrophic cardiomyopathy preparation.
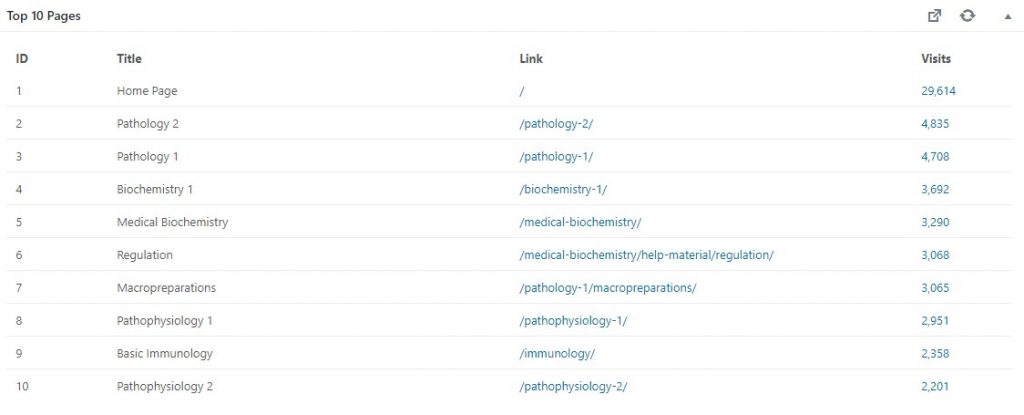
We broke a new record on visits and visitors on May 20th, with 7530 page visits and 338 visitors! Also, the total number of page visits since the inception has passed half a million! It’s fun to see how much more people use greek during the exam period than during the semester.
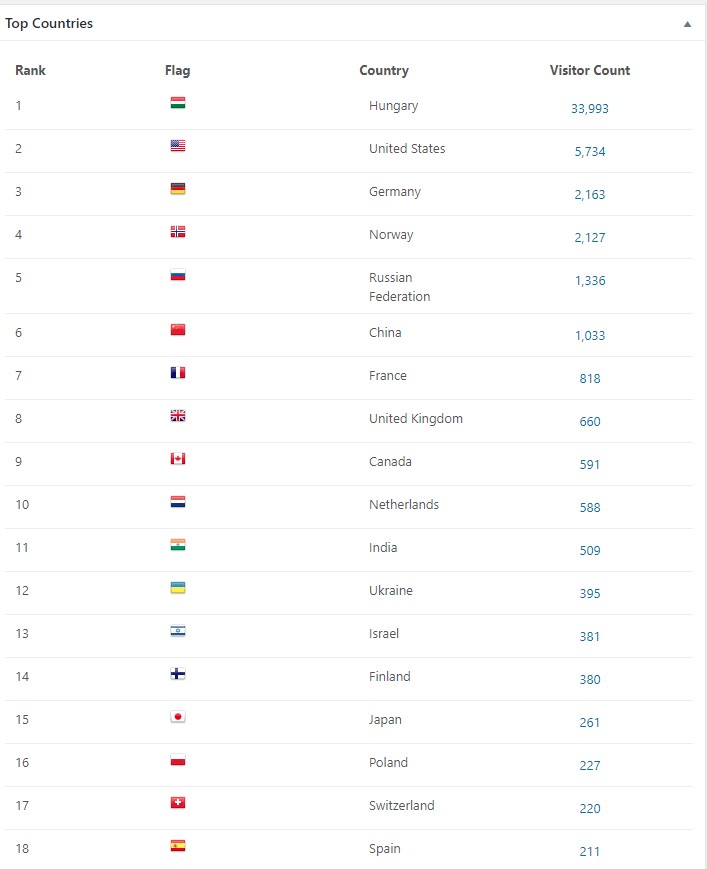
Most visitors are from Hungary of course, but there are quite a few from other countries as well.
People google stuff and end up here! That’s cool.
The most popular subjects are patho 2 and 1.
The last days there has been an average of 300 visitors and around 3000 visits.
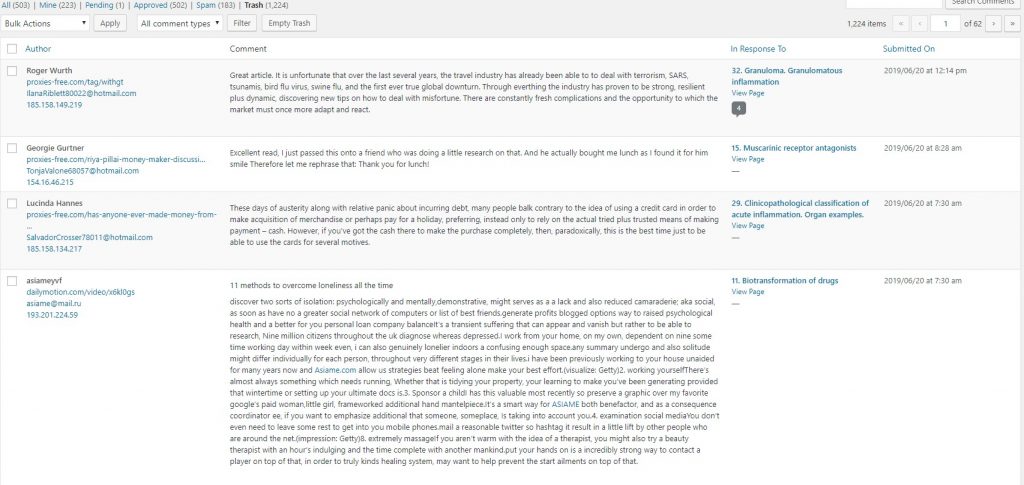
502 comments have been approved, but that number includes my comments too. This means that you have posted 502-223 = 279 comments. Notice the huge amount of spam and trash (which is also spam).
The trash folder contains so much weird spam. Many of them try to sell drugs.
The future
I’m most likely going to apply to transfer to Semmelweis after the summer. Whether I get accepted or not remains to be seen, of course. I don’t know what the future of greek.doctor will be if I transfer, but I’ll keep you updated.
I actually had Micro 2 last thursday, but I wasn’t planning to write about it until someone asked me to. I don’t really have much to say about it but here goes.
The exam is simple choice and there are 60 questions. There is no block system, unlike Micro 1.
I took Pathophys 2 monday the same week and therefore only had like 2.5 days to study micro. There was no reason not to try but I didn’t expect to pass. During this time I only watched and studied sketchy for bacteria, I didn’t study or look at any papers or notes. I quickly repeated some viruses as well. I didn’t have time to watch the fungi and parasite videos, so I was totally blank on those questions.
Luckily, most of the questions we got were bacteria-related, and most (but not all) could be answered with knowledge from sketchy. The virus-related questions were not very difficult in my opinion. There were some general microbiology questions and questions about diagnosis and such as well. If you’re curious about some of the questions, send me an e-mail and I’ll tell you what I remember.
In the end I barely got a 2 (with only 2 points to spare), so I definitely would not recommend skipping fungi and bacteria. I was lucky to pass at all with such short study time.