This is the link to this semester’s notes and Anki. The only notes there are neuro 2, and I probably won’t write for any other subjects. The neuro 2 notes are getting close to finished. When they’re almost finished, I’ll upload them to the website like normally, and do the last edits directly on greek.doctor.
For the first time, I’m making Anki flashcards. I’ve made flashcards in these subjects:
Nephrology – based on lectures and seminars
Neurology 2 – based on my notes
Paediatrics 2 – based on questions
Infectology – based on lectures and seminars
Psychiatry (same questions as last semester)
You’re welcome to use them if you want. Every time I add new cards I create a new file in the folder. Download the file and import it, and the new cards will be added to your Anki.
I didn’t do any pranks for april 1st this year, but I wanted to do something fun anyway. Every day greek.doctor receives many spam comments, mostly phishing ones which try to trick you to click a link in the comment. I thought it’d be fun to reply to those comments as if they were real.
Many of the spam comments are obviously targeted for personal blogs and politically motivated ones, which greek.doctor are not, which makes for some funny situations where the comments are very unrelated from the topic they’re commenting on. Some comments are very generic and could fit virtually any personal blog, some try to push medications or vaping, and some push explicit services.
I’ve edited out the phishing information from the comments by replacing them with XXXXX. The topic they’ve commented on is at the top of each picture.
This is the moment at least two of you have been waiting for for almost a year! See also the previous post if you’d like to compare.
Page visits
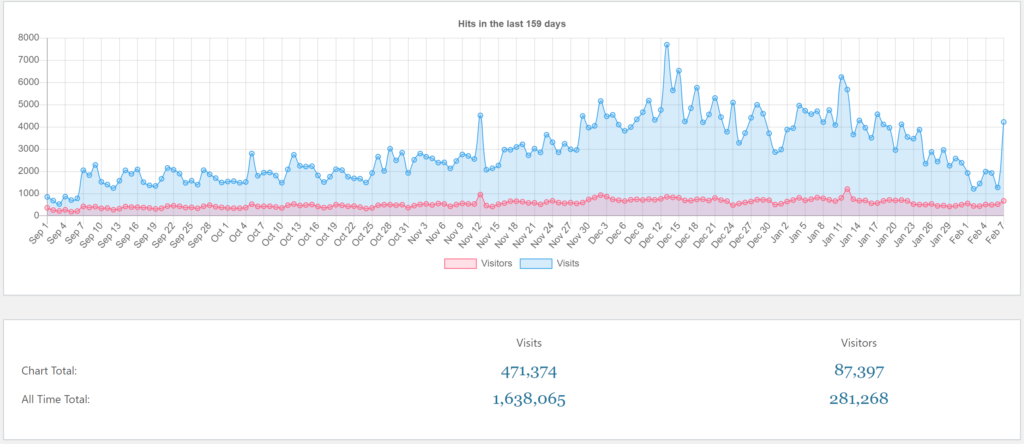
As usual, a page “visit” refers to opening a single page on greek.doctor. A “visitor” is a unique person within that day.
These are the page visits for this semester, which began at September 7th, and a few days preceding it. Not surprisingly, the numbers are lower in the days preceding the semester, at around 200 visitors and 800 visits per day. Then, the semester began at September 7th, after which visitors numbers and visits suddenly increase to around 400 visitors and 2000 visits.
There is a very nice sinusoidal pattern in the first weeks of the semester, with much higher visitor numbers and visits on Monday – Wednesday, with numbers dropping off the rest of the week until the next Monday.
Visitors and visits remain relatively stable in the first 7 weeks, as people are generally on low gear in the first half. Classically, people start panicking around the 7 week mark, after which a higher gear is assumed.
There is a small peak at November 12th, but I don’t know why. I don’t have good insight into which pages were actively used during that day, but I think pathophys pages were most active. Could it be the day before pathophys 1 midterm? Was there even a midterm this semester?
Page visits peaked during this period on December 13th, at 7701 visits, the day before the beginning of the exam period. I’m certain that more cramming of information occurs on this day than on any other day of the exam period or semester. And then, in the afternoon hours of December 14th, most of the information was probably forgotten.
Page visitors peaked on January 12th, for reasons I don’t know. There were 1204 visitors that day.
Numbers were low at December 31st and January 1st, at 3000 visits and 500 visitors.
Since last post, we’ve passed 1 000 000 page visits, and we’re already over half way to 2 million!
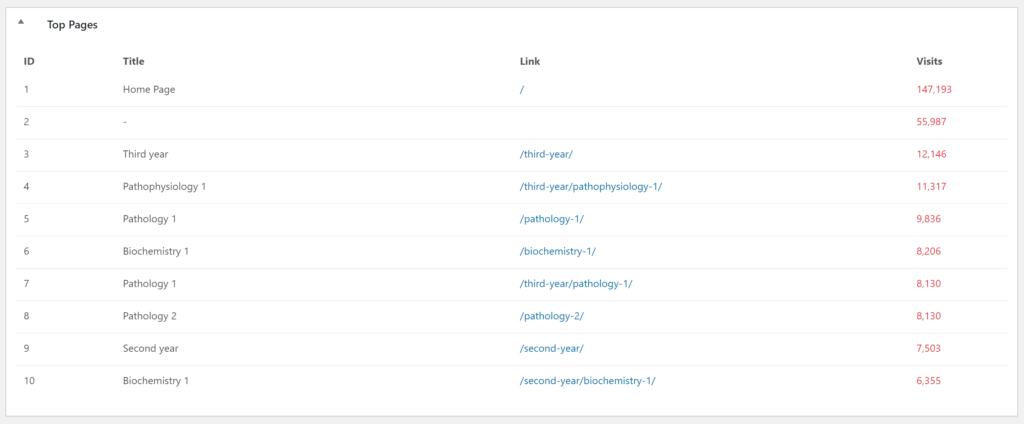
I think it’s safe to say that the notes for third year subjects are the most popular. These numbers only account for the visit to the parent pages of each subject, not the child pages of each subject. The results are kind of messed up because I moved all subjects to their respective years sometime during the summer (I think?), which is why you see both /pathology-1/ and /third-year/pathology-1/ in this list, even though they’re the same page.
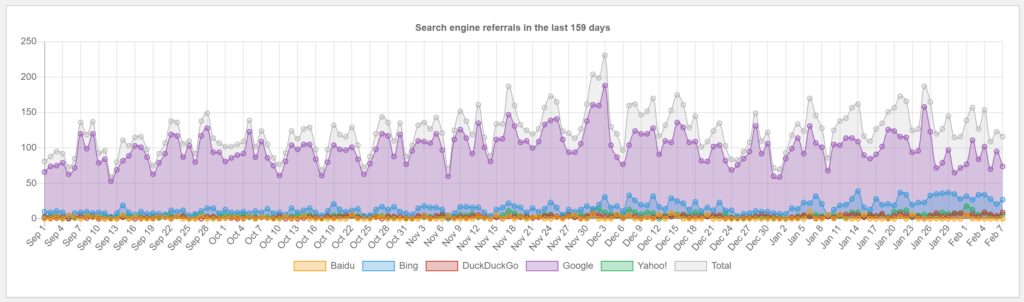
Looking at the number of page visits from search engines is fun, because there’s a much smaller correlation between them and the semester at POTE than there is for other metrics. I assume this is because most POTE students don’t use a search engine to find greek.doctor. Most search engine referrals are from people searching for medical terms and ending up here.
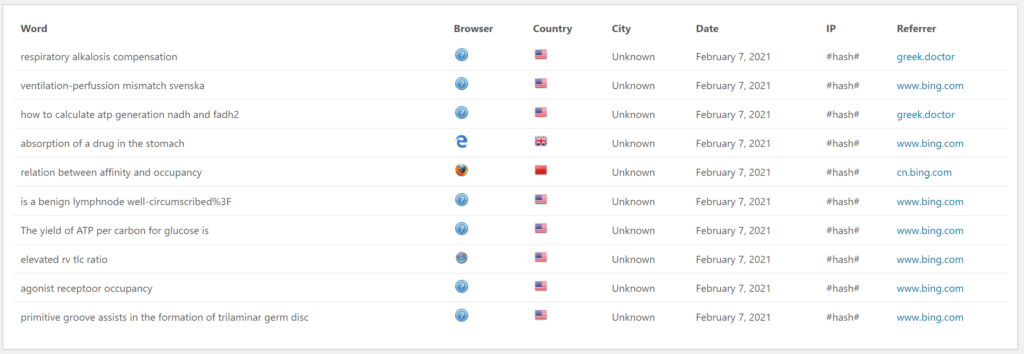
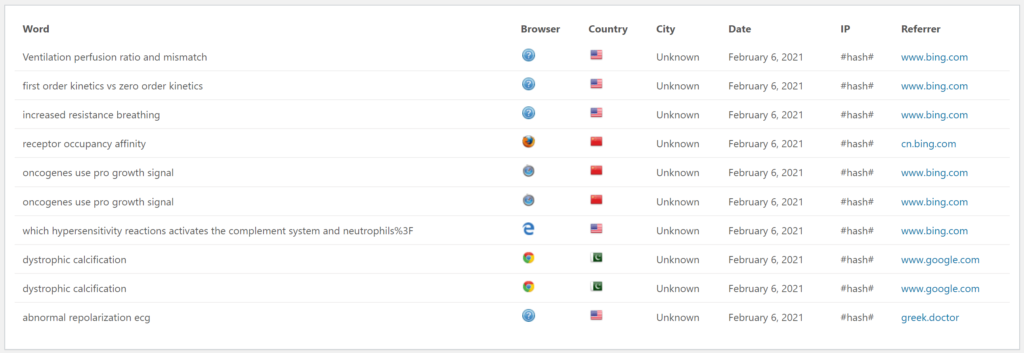
There are the last 20 search words people used before ending up at greek.doctor. This is one of my favourite metrics; I love looking at what people are looking for before ending up here. I hope they find what they’re looking for.
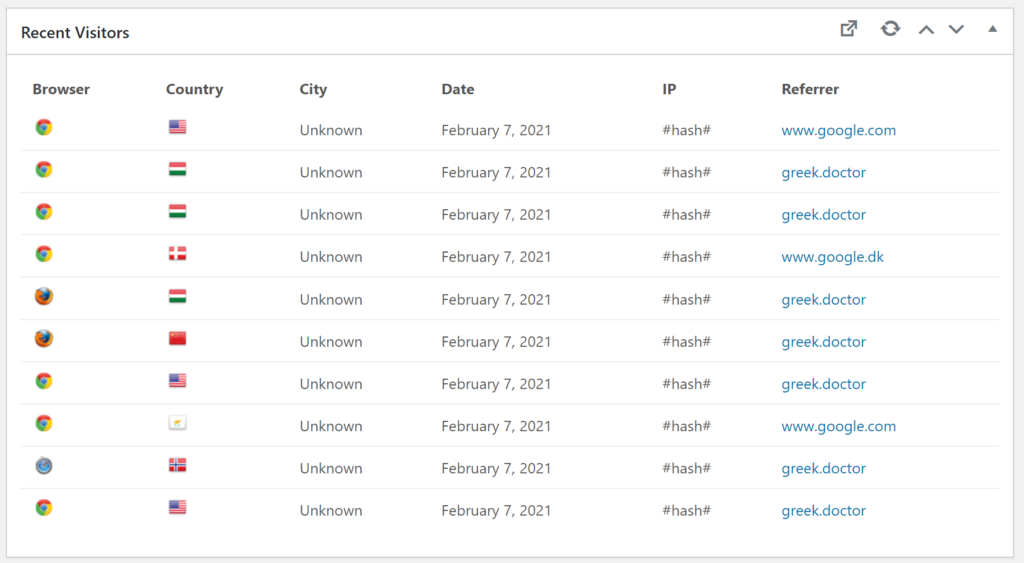
These are the countries from where the last 10 visitors were from. There is a bit of variety, which is cool!
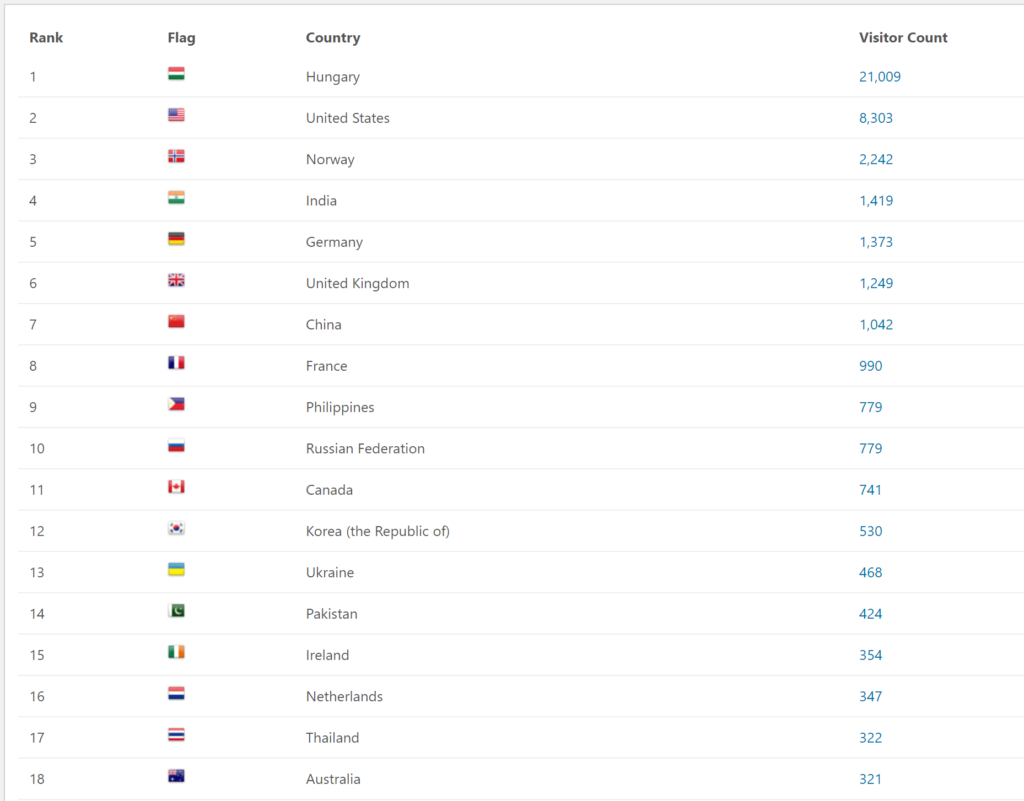
This list shows the number of visitors from each country during the semester.
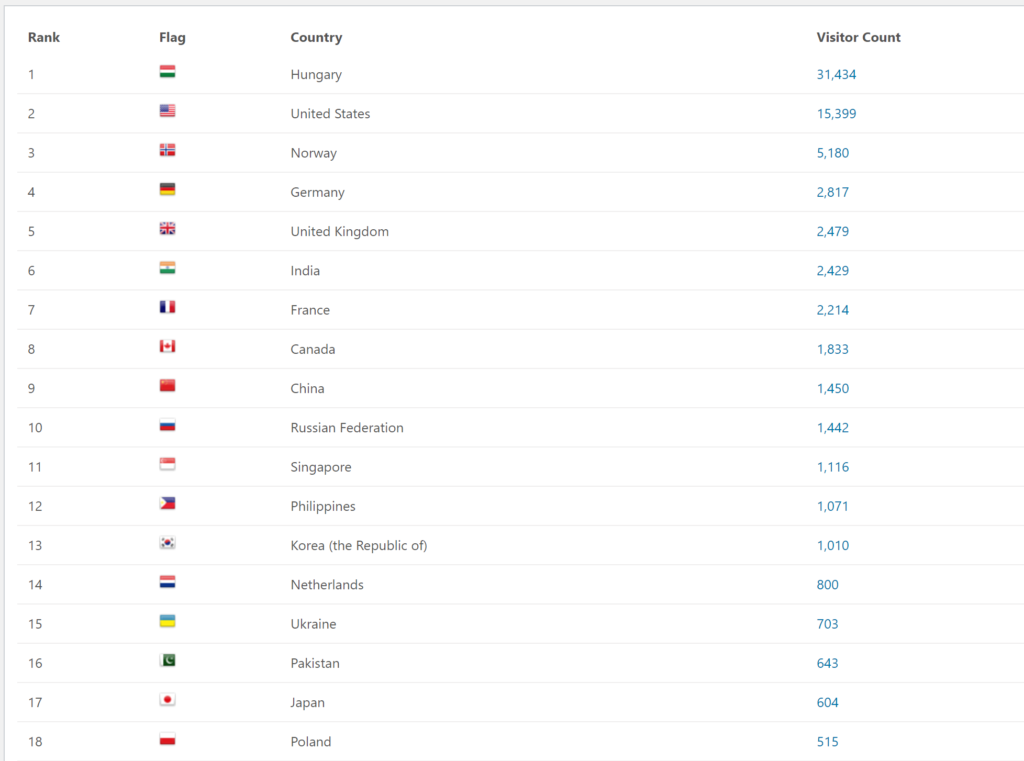
This list shows the number of visitors from each country during the exam period. It’s very interesting to see the large variety, although it’s no shocker to see that Hungary is at the top by a large margin. Hungary would probably have won by an even larger margin if most of us didn’t travel home to have our online exams from home.
Comments
It’s time for a few comments! There are now 1362 comments, of which 600 are mine, leaving 762 comments for others.
Important discussions in the comment section. From here
Fun fact: I initially wanted to study in Germany, for which you need to pass a B2 level German exam. I learnt German but in the end only passed 1/4 language exams, causing me to end up in Hungary. Damn you past me for not studying German enough! From here
I don’t think many people have heard of the Marvel super hero Ball Fondler. The name is unlucky but when his first comic was released in 1986 testicle fondling wasn’t invented yet so the term referred to fondling of golf balls. True story! From here
Maybe they thought I’d hear their comment better? From here
Results of maintainance
Maintainance went pretty smoothly. Some technical jargon ahead:
The server was running ubuntu 16.04, which was EOL soon (April?). It’s now upgraded to 20.04, which is supported for 4 more years. I’ve also hardened the server a bit. I was planning to make a good automatic backup solution during the maintainance, but there wasn’t enough time for me to finish it. That shouldn’t require downtime, though.
Next semester
I don’t know which subjects I’ll write notes for this semester yet. I’ll let you know, though.
I need to do some maintenance work on greek.doctor. However, unlike Neptun, I’ll try to do it when the website is not in heavy use. So, I’m scheduling maintenance for:
Friday 5th of February at 17:00 to Sunday 7th of February at 23:59
That’s at the end of the extra exam week, so no one should need greek during those days.
This is the first time I do this, so I have no idea how long it will take, but I don’t think it will actually take that long.
I’ll wait with the statistics until after the maintenance, in case anything interesting to write about occurs during the downtime.
So I had paeds 1 yesterday. The day before, at around 9:00, everyone who were to have the exam got an email stating the examiner and the time of everyone’s exam. Our examiner was to be Dr. András Tárnok, and my time was 9:10. According to the email, we were to call the examiner at our designated time. There were 20 minutes between each student’s time, so we knew upfront that each exam would last maximum 20 minutes.
So 9:10 yesterday, I called him on Teams, and he answered. He asks my ID, which of my names to use and whether I’m in Hungary.
He holds up the cards with the neonatology topics in a fan-shape. He asks me where to pick from. I tell him to pick somewhere in the middle, and out comes the first topic: “Persistant pulmonary hypertension of the newborn. Patent ductus arteriosus.” He asks me if it’s alright, to which I reply that it is.
Examiner: Can you start with the second part? Patent ductus arteriosus?
Me: Okay, so the ductus arteriosus is an embryonic structure which connects the truncus arteriosus with the aortic arch, so it allows blood to avoid the lungs in embryonic life. Persistant ductus arteriosus is when it doesn’t close early after birth.
*During these sentences he was writing something down, so he didn’t notice, or at least react to, my mistake regarding truncus arteriosus.*
E: So is it good or bad?
M: It’s not good, because, if it’s very small it might be asymptomatic, but if it’s large it may cause symptoms.
E: What symptoms?
M: For example, uhm, dyspnoea, or tachycardia.
E: Okay.. Please tell me, where is this little blood vessel? What does it connect to?
M: It connects the truncus arteriosus to the aortic arch.
E: Truncus arteriosus?
M: No, no, the pulmonary trunk, sorry.
E: So there’s a connection between the pulmonary artery and the aorta. Now think about it, if you have a connection between the systemic and the pulmonary circulation by this little thing, what is going to happen?
M: The pressure is higher in the aorta, so it’s like a left-to-right shunt.
E: Okay, so what’s going to happen with the lungs then?
M: They will experience more blood than they normally do
E: So then what is going to happen?
M: Pulmonary hypertension.
E: Good. Do I need to ask questions or would you like to make sentences yourself?
M: Well, I can try to make sentences but I appreciate some help if I need it.
E: You’ve already received help. *we laugh*
M: Yeah, so this is not a good thing, pulmonary hypertension is not a good thing. Uhm, where should I continue. It can be closed either pharmacologically or by percutaneous procedure. Pharmacologically you would use an NSAID like indomethacin or ibuprofen.
E: Okay. Why do we indomethacin?
M: It works because prostaglandins are what keep the ductus arteriosus open
E: It’s much nicer to have it explained like that, so if you now it, just say it so. It’s so easy. Prostaglandins are what keep it open, so if I give something which inhibits prostaglandin synthesis, it will close. If that doesn’t help, we have the surgical option. If not percutaneous we must perform a thoracotomy and put a clip on there. Good. Clinically, what do you see apart from tachypnoea, or whatever. Is there anything else on physical exam?
M: Uhm, they may experience respiratory distress.
E: Is it the cause or the consequence?
M: The consequence.. Uhm, on physical exam there is a murmur.
E: Okay, we’re approaching. Tell me the characteristics of that murmur.
M: I can’t recall actually..
E: When do you hear it?
M: After systole, I would suppose…
E: Where does this murmur generate?
M: Where? Oh, uhm, I would guess the turbulence in the pulmonary trunk?
E: Ehm, we’re going down to basics, to year three now. So if we do auscultation at the heart, you know that different sounds are produced in different cycles of the heart-beat. In this scenario, what do you think?
M: Second heard sound?
E: What is the problem [of the PDA]? Nikolas, tell me. Where is the problem?
M: The problem is the pulmonary hypertension.
E: No, the problem is the connection between the two circulations by this tiny little blood vessel. This is the problem, this is the PDA, yeah? And where is this?
M: Between the aortic arch and the pulmonary trunk.
E: Is it outside or inside the heart?
M: Outside.
E: Okay. Does it have any connection to the valves?
M: Uhm, no, not directly.
E: Okay. So if it’s outside the heart, and it’s not connected to the valves, then what is the characteristics of this murmur? Because, in the heart, if we have a systolic murmur, or a diastolic murmur, it is connected to the phase where the heart is beating. And because the valves are open and then closing, this is going to give you the first and the second heart sounds, yeah?
M: Yeah
E: Now, this tiny blood vessel has no valves in it at all. So, how would you characterise it?
M: Uhm..
E: Does it have any relation to the heart cycle?
M: Oh, uhm.. no, I would suppose not.
E: No. So, what is the charactisterics of this murmur?
M: So it’s constant throughout the heart cycle.
E: It’s continuous. Because it is going to happen all the time, from the high-pressure area to the low-pressure area, and you will hear this sound because it’s a thin connection, therefore, when the blood is flowing through a narrow part, it is going to produce the sound. Where do you hear this? Is there a typical site where you can hear this?
*Somehow it just occured to me*
M: In the left infraclavicular region.
E: Exactly, exactly. So if you suspect it you put your stethoscope there, and you try to hear. It’s called a continuous type of murmur. It doesn’t have an end, because there’s no valve to put an end to it, where the blood flow is stopped. Okay?
M: Yeah.
E: Okay, so now that I’ve explained you this topic, we need to move on to the second one, I don’t want you to get in trouble with the persistent pulmonary hypertension, okay? I do not wish to explain more of that. So all-together this is a 3 at the moment.
Not a great performance by me thus far, but he’d been very nice about it. We were around 11 minutes into the exam. He hold up the topics for general paediatrics and asks me where to draw from. I ask him for a card from the middle again, and he draws out the second topic, “diabetes mellitus”. “Is it better?”, he asks. “That is better”, I reply.
E: Now. No interruptions, nice sentences, brief summary.
M: Okay, so. In childhood, still diabetes type 1 is the most common, but of course type 2 is becoming more and more common, but I’ll focus on type 1. So type 1 is mostly an autoimmune phenomenon, where there’s autoimmune destruction of the beta cells causing them to have insulin deficiency. There are many antibodies involved in this, like anti-insular cell, anti-… Oh, well I guess I just remember that one. Glutamic acid something, there’s an enzyme, GAD or something. Okay, anyway. So a child may present with typical symptoms of diabetes type 1, or they can present with ketoacidosis. The typical symptoms of diabetes type 1 are weight loss, polydipsia, polyuria.
*He hold up three fingers*
E: Another “p”. [Like, another symptom on “p”]
M: Uhm..
E: They eat a lot.
M: Sorry? [I couldn’t hear what he said]
E: They eat a lot.
M: Polyphagia.
E: Exactly.
M: Yeah, they have to make up for the lost glucose. And weight loss, even though they eat a lot. Or maybe they wouldn’t gain as much weight as their eating habits should’ve made them.
*He nods*
M: Okay, where was I? Symptoms, uhm.. So, the diagnosis can be made in multiple ways. Fasting plasma glucose, HbA1c, OGTT, random plasma glucose.
E: Okay.
M: So if the HbA1c is above 6,5%, or the fasting is above 7 mM, or the random is above 11,1 mM, or the OGTT is above 11,1 mM, all of those are diagnostic for diabetes.
E: How do you determine that there’s no insulin?
M: You look at the C-peptide level.
E: What is that?
M: Sorry?
E: What is the C-peptide?
M: The C-peptide is the peptide which is released simulatenously as insulin from the beta-cells.
E: How? *slightly dissatisfied face*
M: No, it’s actually a part of the prepeptide of insulin, which is cleaved off to make the C-peptide and the insulin.
E: How? Once a life I give an injection and it’s done?
M: Sorry?
E: Is it like a jab? I give it once a life and it’s done?
M: No, it’s daily. There are multiple regimens to do this. They often use once or twice a day a long-lasting insulin, and before meals that can take some short-acting insulin.
E: Where do you give it?
M: You give it in the abdominal fat.
E: So how is it administered?
M: With, uh…
E: Or *where*?
M: Oh, subcutaneous.
E: Yes, okay. Why don’t we give IV?
M: Well it’s because it’s much easier for the patient to inject themselves subcutaneous than IV.
E: And, also? What is going to happen if you inject IV?
M: Everything is immediately into the blood stream, so it won’t be released gradually from the subcutaneous fat.
E: Okay. What is the prognosis of this medical condition? Are they going to be cured, ever?
M: No, they’ll never be cured. They have to do this life-long. And the exact prognosis depends on how strict they are with maintaining normoglycaemia to the best of their ability. Most of them will develop some diabetic complications, microvascular or macrovascular. Diabetic retinopathy, neuropathy, nephropathy.
E: Have you ever seen a type 1 diabetic patient?
M: I have some friends who are, but I’ve never seen it in a patient, no.
E: And your friends, just a personal question. Are they all right?
M: Yes, they are.
E: So they’re functioning well?
M: Yeah.
E: And that is the aim of the treatment. To have a normal life, kind of. What about restrictions in this medical problem?
M: So they should try to eat almost a constant amount of carbohydrates, because the amount of carbohydrates they eat must be balanced out with the insulin they take.
E: Okay. Have you heard of insulin that is somehow acting differently than the normal? That has an advantage nowadays in diabetic patients.
M: Are you talking about like a pump?
E: Pump is okay, yes, but anything else you have heard? Because you said, it has to be given the short-acting before the meal, yeah? What if I don’t feel like eating? I’m not hungry. And the insulin is already in my body. What’s going to happen?
M: You would get hypoglycaemia.
E: Can you give me any ideas what it can cause?
M: In the worst case it could cause a coma, but in …
E: And death.
M: And death, yeah.
E: So you lose consciousness, you’re going to have seizures. And you lose contact with the environment. Now, have you heard about so-called insulin analogues?
M: Yeah.
E: Insulin analogues are good because you can give them after the meal, because they’re much faster. So it can be paired with the carbohydrate input. So if you don’t know, because you have a bit of tummy pain or sickness-feeling, and you don’t feel like eating that much, you can balance it to the amount you have eaten. And it’s not going to disturb your blood sugar level that much. Okay. All right. Nikolas. That was 5. I’m happy. So all together, it’s a 4. Okay?
M: Okay, yeah, I think that’s deserved.
[I meant to say that that’s more than I deserved but I was so nervous and said the wrong thing]
E: Okay, Nikolas, please look at those neonatal stuff, because we can lose patients with persistent pulmonary hypertension, or not discovered PDA can cause long-term problems. It’s a significant question which you’re going to fail at the final if you have big gaps, okay?
I said thank you, we wished each other a good day, and with that I was done with this exam period.
He was very nice and compassionate, and was smiling and nodding along during the whole exam. I’m glad I had him as my examiner, although I’ve heard that all examiners in paeds are very nice.
I had an amazing idea before this exam. I’d start an exercise session on my smartwatch so I could monitor my heart rate during the exam. I had to choose the type of exercise. I chose “gardening”, because “having exam” was not an option for some reason. Here are the results!
“Du gjorde litt ekstra!” means “You did a little extra!”, which is nice.
My “gardening session” started 08:56, 14 minutes before my exam started, so the exam started 14 minutes into the gardning. At that point, my heart rate peaked at a comfortable 155 bpm. I suppose the sudden drop was because of how calming the examiner was. I don’t know what happened toward 24 minutes; the HR sensor probably dysfunctioned. At around 25 minutes I drew my second topic. At around 33 minutes my exam was done. Fun stuff!
Now that I’m done with my exams I’ll upload my neuro and paeds 1 notes to the website as usual. At the end of exam period I’ll return with the fan-favourite: statistics (I promise!).
Good luck to those who aren’t finished yet, and congratulations to those who are finished!
So I had obgyn 1 yesterday. The day before me and the other 14 students who had the exam were added to a new team on teams. There, the secretary Dora Szigeti wrote a message that at 8:00, we would receive our topics, and when it was our turn, the examiner would call us. Another student asked her who our examiner would be, and she answered “Dr. Bálint Farkas”.
At 8:00 the next day, we all joined the meeting. There, the secretary gave us some more information, about how all students will at least get 30 minutes preparation time. She then drew one A topic and one B topic for each of us, in alphabetical order by last name. I was the eighth student to draw topics, so I knew I would be the eighth student to have the exam as well.
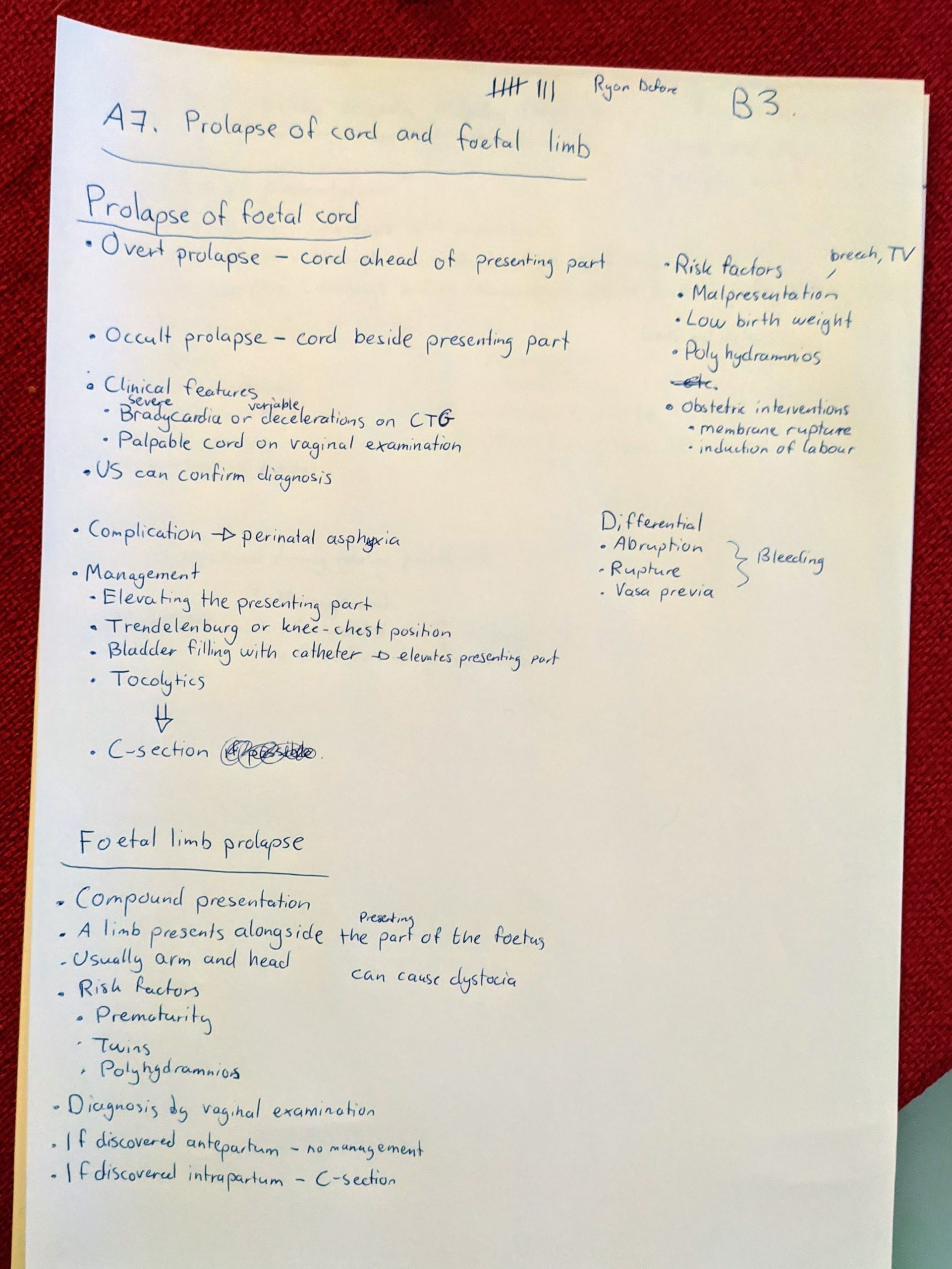
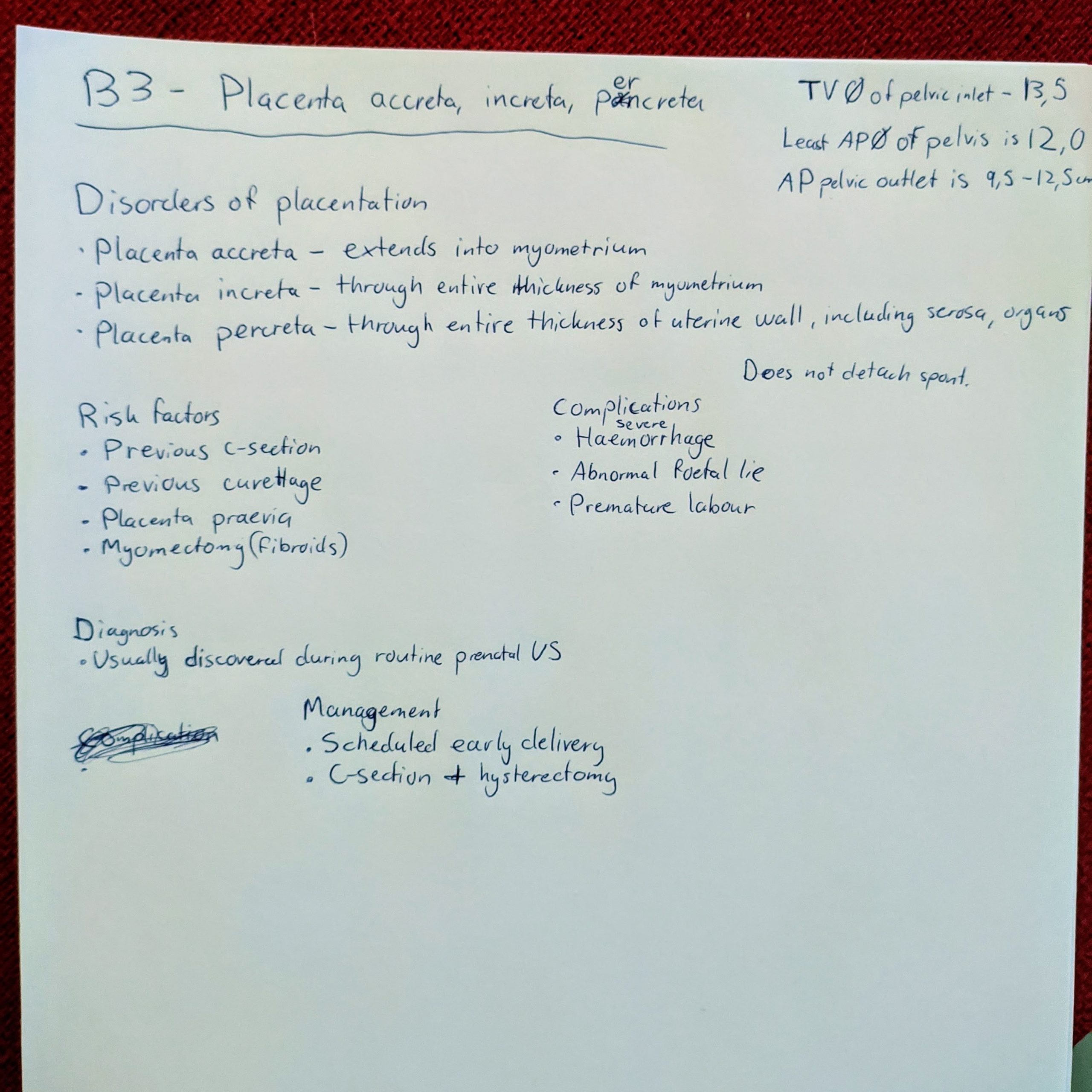
My topics were: A7 – Prolapse of the foetal cord and limb, and B3 – Placenta accreta, increta, percreta.
She told us that while we prepare we must leave our cameras on but microphones off, and we could leave the room and eat and drink as we wanted, no need to ask for permission.
Because I knew the alphatical order, I could tell when my turn was coming up, which was nice. I was the eighth student, so my exam began at 10:40 when Dr. Bálint Farkas called me. He began asking for ID, and then left me to explaining my topics. I began with my A topic.
I began by telling him everything I’d written about umbilical cord prolapse (except the differentials). After I’d mentioned perinatal asphyxia, right before I was going to mention the management, he asks “What would you do about it if you diagnosed this on the labour ward. What would be the management?”. I continued with what I’ve written about management. He said “OK”, so I continued on with what I’d written about foetal limb prolapse. He said “OK, next topic”. So there were no questions to this. I continued on with my B topic.
I’d written the pelvic diameters in the corner because I’d heard that someone else was asked about that before me.
I tell him everything I’d written. He had no questions to this topic either, but began asking me general questions, where my performance wasn’t exactly excellent.
Examiner: Can you tell me other causes of postpartum bleeding?
Me: Uterine atony, is the most important cause.
*I couldn’t recall any other causes*
E: What does “cotyledon retention” mean?
M: It means that one or more cotyledons have been retained in the placenta (I meant to say uterus), so that not all of the placenta has been expulsed in the third stage
E: What is uterine inversion?
M: It is when the uterus sort of prolapses out of the cervix
E: Can you tell me a reason for that?
M: I don’t know a reason for that.
E: It can be artificial if you pull the cord without the placenta detached, so it brings the uterus with it, or if the cord is too short, so it pulls the uterus with it. It’s very painful and causes very heavy bleeding.
E: What is the so-called Crede manouevre?
*He actually sent me the word “crede” on message because I couldn’t understand the word*
M: Is it the one where they return the inversed uterus?
E: No.
M: Then I don’t know.
E: It’s a maneouvre to fascilitate the detachement of the placenta through the abdominal wall. You squeeze it out like a plum.
M: Okay.
E: Do you know what the Ritgen maneouvre is?
*Once again he sent me the word “Ritgen” on message*
M: No, I don’t recognize that name either
E: So you’re not really a maneouvre guy, are you?
*We laugh*
E: Okay. It’s when you grab a sterile towel and hold the perineum when the head is deflexed to protect the perineum.
M: Okay, I had heard of that, I just didn’t know the name.
E: What is an episiotomy by the way?
M: It is when you cut the perineum to increase the opening of the birth canal, either midline or slightly oblique.
E: Yeah. How many stages of layer do you know?
M: Four.
E: How many movements does the foetal head do during normal labour?
M: So it begins with descent, …
E: No
M: Engagement, descent, and flexion at the same time?
E: Flexion, okay.
M: Yeah flexion, and then internal rotation, and then the head extends out of the birth canal, and then the external rotation back, and then the anterior shoulder and then the posterior shoulder.
E: Yeah, okay. What is shoulder dystocia?
M: It is what occurs if the shoulder has not been born, so to say, in the same contraction or the contraction after the contraction where the head was born. So it’s a form of mechanically obstructed labour.
E: What can you do about it?
M: Operative delivery, so foreceps or vacuum
E: No, the head is already out.
M: Oh no, yeah of course. You do the, uhm.. I don’t remember the name of this maneouvre either, but you pull the legs of the mother, and put pressure on the pelvis somewhere, to try to help the shoulder out.
E: So where would you put the pressure on the pelvis?
M: On the symphysis
*I was only half-sure that symphysis was the right answer, which is why I didn’t specifiy where to put pressure initially
E: On the symphysis, yeah? To remove the stuck shoulder. The manouevre is called McRoberts. What if that doesn’t work?
M: I remember there’s a list of possible managements. I don’t think.. You can also cut the clavicle or the symphysis of the mother, but I don’t think that’s the next stage..
E: Those are drastic movements …
M: Yeah, there is another movement you would rather do before that.
E: Cutting the symphysis of the mother, wow. Cutting the whole urethra and bladder and everything. That’s a bloodbath, man.
M: Yeah..
E: I mean, one of my collegues who retired like 20 years ago told me about how they used to do that in the 1970s, but I haven’t seen it before.
M: I’m glad. I just remember that it was mentioned on the lecture. Uhm.. I’m drawing a blank. I remember there’s a different maneouvre but as we established I’m not good on manouvres.
*We laugh*
E: Yeah. I’ll give you a 4, okay?
M: Yeah, I’m happy with a 4.
E: It wasn’t bad, but it wasn’t excellent, yeah?
Completely deserved, although it’s annoying that they mention procedures on the lecture which apparently haven’t been used for 50 years.
My whole exam lasted 10 minutes. I spent almost exactly 5 minutes with my topics, and the remaining 5 minutes were used to uncover how little I knew about manouvres.
Either way it was a pleasant experience. He can sometimes seem a little intimidating but I was much less nervous during the exam than I was while waiting for it.
My last exam is paeds 1, on Friday. Looking forward to being done!
I had neuro 1 on Monday. I’ve been taking some days off after that.
As we all know, this year we’re having the exam with our own teachers in neuro 1. As such, the procedure of the exam, and what they’re focusing on, probably varies from teacher to teacher, although I’m sure they’ll all be lenient at the exam.
My teacher and examiner was Dr. Márton Tóth, who’s a very sweet and fun man. The day before the exam he told the 12 of us who were to have the exam that day to make groups of 3. The first group of three would start at 10:00, the next group of three at 11:00, and so on. That way everyone knew approximately when their exam would be. Why can’t all oral exams do this?
I was in the first group, so at 10 me and the other three students in the first group joined a meeting our teacher had made in the team we usually used for seminars. He told us that we’d get 4 questions from A and B topics, and one question from C topics. He’d told us beforehand that he feels that the topic list is too extensive for this semester, and so he wouldn’t expect much from C topics.
I volunteer to start, so I do. He begins asking:
Examiner: How do you examine the vision?
Me: You could use a Snellen chart if you have it available, but if not you could hold up a certain number of fingers at 5 metres distance and ask if they can see them. If they can’t, move closer and repeat.
E: And what do you do, if at one metre, there is no response? If at zero metres, there is no response? What should you use?
M: Just a simple light, to see if they can detect light at all.
E: The so-called candle test, yes. Good, okay.
M: Please tell me which pyramidal signs you know.
E: The most important is the Babinski, but also the triflexion response, achilles clonus, patellar clonus.
M: And in the hand?
E: I don’t remember the names, but it’s the one where you flick the fingernail.
At this point he asked the next student if they remembered the names of the two pyramidal signs of the hand, but they didn’t either.
E: Okay. Other pyramidal signs?
M: Do you mean upper motor neuron lesion signs in general or pyramidal signs specifically? I know upper motor neuron lesions like spasticity, no atrophy, hyperreflexia …
E: What does hyperreflexia mean?
M: It means that the response is stronger than usual, or the reflex zone is larger, so you can elicit the reflex at a larger area.
E: Okay, okay. How do you examine muscle tone?
M: Okay, so we start for example in the upper limb. We can begin with moving the elbow joint, feeling for flaccidity, rigidity, or spasticity.
E: Okay. Which type is which? How can you describe them?
M: Flaccidity is when there is a loss of muscle tone, so the resistance to passive flexion is decreased. Rigidity is a constant, non-velocity-dependent resistance. Spasticity is a velocity-dependent, so that if you do it quickly there is less resistance, and if you do it slowly there is more resistance. The clasp-knife phenomenon is characteristic for spasticity, where there initially is a lot of resistance which suddenly releases. After the elbow you would continue with the wrist …
E: It’s enough. Please tell me which levels of vigilance you know.
M: So after normal we have torpidity …
E: No, torpidity is not that. Vigilance.
M: Okay, so somnolence.
E: Yes!
M: Somnolence is when the patient is sleeping but can be awoken, but after you have stimulated them they fall back asleep. You have sopor, which is deeper, where you can only awake them with a stronger stimulus, like shouting. You have stupor, which is even deeper, where you need strong pain to wake the patient. Then you have coma, where no stimulus would wake up the patient.
E: Okay. For C topic, you can choose stroke, epilepsy, or Parkinson disease. Which do you want to talk about?
M: I can do Parkinson disease.
E: Okay, tell me something about Parkinson disease.
M: Okay, so the characteristic features of Parkinson include bradydiadochokinesia, hypokinetic gait, micrographia, resting tremor, poor postural stability.
E: That’s okay. There’s idiopathic Parkinson disease and Parkinson-plus syndromes. Do you know the difference between them?
M: Parkinson disease is idiopathic, while in Parkinson plus syndromes you have Parkinsonism plus other clinical features. We have for example Lewy body dementia and corticobasal degeneration. In Parkinson plus syndromes there is less response to dopa therapy.
E: So what are the plus symptoms of Lewy body dementia?
M: They have dementia, and disinhibition?
E: Nono, they have hallucinations.
M: Oh, yes, yeah. Hallucinations.
E: Okay, you told me about corticobasal degeneration. What are the plus symptoms of it?
M: I think they have dementia as well, but I don’t remember other plus symptoms.
E: So cortical degeneration. What happens when the cortex is degenerated? Focal or Broca area, for example. (Pointing to his Broca area)
M: Aphasia?
E: Yes. And here (pointing to his temporal lobe I think)?
M: Uhm.. Apraxia, maybe?
E: Yes. Lobar symptoms. It is very logical. Now you are learning. Okay, so we have two Parkinson plus syndromes, what is the third one?
M: Uhm.. (I don’t remember the last two).
E: You’re very good until now!
M: I don’t think I remember the last two.
E: Nono, this is not a good strategy. (We both laugh). This is not good. Never say that. Okay? Can you remember?
M: *thinking*
E: Earlier name was Shy-Drager syndrome..
M: I haven’t heard that name.
E: There is a Hungarian link, because this professor was working together with professor Komoly in this department, so everybody here knows it very well. It’s multiple system atrophy. There are three subtypes, do you know them?
M: 🤷♂️
E: MSA-C, MSA-B, and MSA-A. Do you know them?
M: No, I don’t think I do.
E: It’s no problem. And the last one?
M: 🤷♂️🤷♂️
E: Can I help you?
M: Yes please.
E: The patient is unable to gaze downwards. The vertical eye gaze is inhibited.
M: (At this point I’m just pretending to think, because I have no idea but don’t want to tell him that)
E: It was described in Detroit by three people.
M: (This confused me a lot) I don’t think that helps me
E: I’m just joking (we laugh). The last one is progressive supranuclear palsy. Have you slept?
Before the exam period he made a big deal that we must make sure to sleep well before our exams.
M: Yeah, I did sleep! But I’m nervous, so..
E: Never, never.. for me? Never be nervous. Never be afraid. So now you are between 4 and 5. I can ask you one more question for the 5.
M: Yes please.
E: What is the difference between central and peripheral facial palsy?
M: In central the upper part of the face, the forehead and eye-blinking is not affected. The symptoms are contralateral to the lesion, while in peripheral they are on the ipsilateral side.
E: Which muscles are affected?
M: So in both types there is drooping of the corner of the mouth, loss of the nasolabial fold. In peripheral type you can also have hyperacusis and ear pain. The frowning and closing the eyes is impaired. They can’t whistle or blow their cheeks.
E: Okay. Good. Congratulations.
At this point he told me to stay in the meeting while the others had their exam, which was kind of a drag because I just wanted to leave, but there was no examiner and there are rules for witnesses or something. He didn’t say my grade but because he didn’t say anything I assumed I answered the last question well enough to get the 5.
My exam lasted for 13 minutes. The other two students’ exams lasted longer, so that our session lasted over 1 hour total. All three of us got 5, even though all three of us got multiple questions we couldn’t completely answer. Our teacher is a very nice and kind man, both as a teacher and an examiner.
From what I’ve heard, the exams of the different teachers are quite different, so if you can hear the experience of someone who already had your teacher this exam period, that would be the best. Either way, I’m sure everyone will pass neuro 1 this semester.
My next exam is ob/gyn the 4th of January, but I’m taking some days off until then. Good luck!
So I had psych 1 exam today. Yesterday we got an e-mail that the exam would start at 7:30. At 7:45 all of those who were signed up for today were added to a team, and we all joined a meeting with the examiner at the same time. The examiner was Tamás Tényi, and he apologized for the delay.
He wasted no time, asking the first student on the list for their ID as soon as we joined the meeting. After the ID he immediately started asking questions; there was no drawing topics or anything. Each person got 7 – 10 questions. In some cases where people couldn’t answer questions, he asked the same question to another student. These are the questions I was asked, and the answers I gave:
What are the dissociative disorders?
This was a question he’d asked two students before me, who didn’t know the answer
I listed dissociative identity disorder, dissociative amnesia, and depersonalization disorder. He wanted a couple of more, but I didn’t know any more.
What does depersonalization mean?
I couldn’t answer this, but he explained it to me afterward.
If a nurse induces haematuria in herself in order to get admitted to the hospital, what is this condition called?
I said “facticious disorder, also called Münchausen syndrome”
What is the Werther effect?
I said “copycat suicide, where the fans of a famous person takes suicide after the famous person does”
What are the ABC drugs?
I said “I don’t remember the C, but I remember aripipraxole and brexpipraxole”
It didn’t look like he minded that I didn’t know the last one
What is the mechanism of action of the ABC drugs?
I really fucked up here. I completely forgot that they are 3rd generation antipsychotics, so I said that I don’t know. He asked another student the same question, who got it right of course.
Which are the mood stabilizers?
I said “lithium, valproate, lamotrigine, and carbamazepine”
What is the most dangerous side effect of lamotrigine?
I said “Stevens-Johnson syndrome”
And with that, my exam was done, and I got a 4. I timed it, and my exam took approximately 4 minutes. The other people’s exams took a bit longer.
I’d say it’s best to try to keep your answers to the minimum, only answering his specific question and not talking around the subject. He seemed to appreciate short and concise answers.
Since last experience I’ve passed ophthalmology, dermatology, forensic, surgery, gastro, all written. Dermatology and forensic had written chances during the semester for the first time ever. Dermatology was easy, forensic was horrendously difficult. I hope forensic learns not to make the test this difficult for future years.
I finished the first exam of this semester on Thursday. This semester we are so lucky that we have some exams before the exam period (not sarcastic). The exam in “Internal Medicine – Diabetes and Angiology” is actually only about diabetes, and it’s a relatively small exam.
Like all exams for us this semester, diabetology exam was online. The worst part of the exam for me was waiting; we were scheduled to have the exam during the time when we normally had diabetology seminars, which for my group was Thursday 8 – 9:30. So we all had to be ready at Teams at 8 and just wait to be called. I was the very last student in my group to have the exam, and so I was called up at 10:30. That sucked.
Because other groups had their exams earlier in the week, and because we’d talked to 6th year students, everyone knew that this was to be a relatively easy exam, where they ask simple questions. My examiner was Dr. Gergő Molnár. The questions I was asked were also simple:
What are the four diagnostic criteria for diabetes mellitus?
What are the major classes of diabetes mellitus?
Give an example of monogenic type of diabetes
Give some examples of endocrine diseases that could go along with diabetes
Give some examples for medications which could induce diabetes
If you have a patient with type 2 diabetes who receives metformin but has not reached the target HbA1c, and has signs of proteinuria, so we would consider him to have chronic kidney disease, what would the preferred drug class of choice?
Name some examples for SGLT-2 inhibitors and GLP-1 receptor agonists
Give an example of an ultra-long acting insulin analogue
Give an example of an ultra-short acting insulin analogue
You have a patient with multiple daily insulin injections who complains about having high glucose values every morning.
What could be the two causes for that?
How can you distinguish between the two causes?
How would you adjust the dose of the evening NPH insulin if it was the Somogyi effect?
You have a patient who is young and you’re struggling to determine whether he has type 1 or type 2 diabetes because he’s not very lean and not very thick. Which objective measurements could be used to distinguish between the two?
And that were all the questions I got. The exam was recorded, and the recording was 5 minutes and 36 seconds long, so it was a short exam. I answered all questions correctly. He didn’t tell me which grade I got (only that it was very good) but if I got anything other than 5 I’ll rebel.
On Monday at 9 we have written ophthalmology “competition”, and if we do well at that we get exempted from the oral exam. Because I failed derma last year, I also have a written derma “competition” the same day at 11. Then we have forensic medicine written “competition” on Thursday.
Every 60 seconds in Africa, a minute passes. And every 60 seconds in Pécs, someone asks which notes they should use and where to find them.
I’ve written some paragraphs about which subjects to prioritize and which notes to use in the different semesters. I also link to the best notes when possible, to make them more accessible.
Only 2nd year is done so far, but I’ll upload 3rd and 4th soon. You can find the pages on the sidebar.